
Sciatica vs. Radiculopathy: What's the Difference, and Why Does It Matter for Treatment?
Written by Connor Sheeks PT, DPT · Published April 2026 · Last reviewed May 2026
Reading time: approximately 8 minutes
If you've got pain shooting down your leg, you've probably called it sciatica. Your doctor may have called it radiculopathy. Someone else may have said it's a pinched nerve. And if you've looked it up online, you've likely found all three terms used interchangeably — which doesn't help you understand what's actually happening or what to do about it.
These terms are related but not identical. The difference between them is not just semantic — it affects how your condition is diagnosed, which treatment approaches are most appropriate, and what your realistic recovery looks like.
This article breaks down exactly what each term means, how clinicians tell them apart, what causes them, and what treatment actually works for each. Written in plain language, with no assumption that you have a medical background.
What you'll learn in this article
• What sciatica actually means — and why the term is imprecise
• What radiculopathy is and how it differs from sciatica
• What a pinched nerve really means
• How clinicians identify which nerve root is involved
• The most common causes of lumbar radiculopathy
• What treatment approaches have the strongest evidence
• When symptoms require urgent medical attention
What Sciatica Actually Means
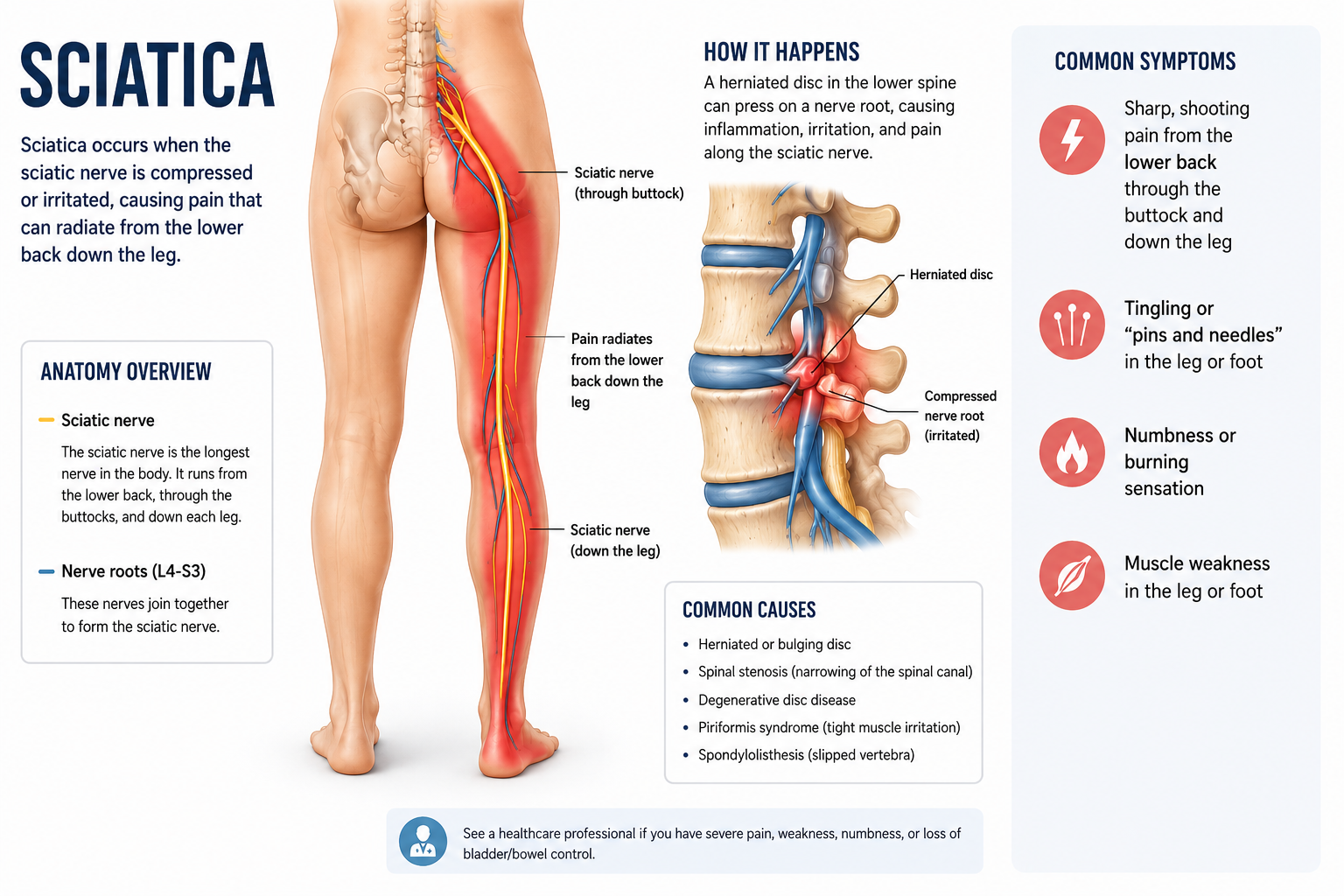
Sciatica is a descriptive term, not a diagnosis. It describes a set of symptoms — pain, numbness, tingling, or weakness that travels from the lower back or buttock down the back of the leg, sometimes as far as the foot — that are caused by irritation or compression of the sciatic nerve or its contributing nerve roots.
The sciatic nerve is the largest nerve in the body. It forms from nerve roots at the L4, L5, S1, S2, and S3 levels of the lumbar and sacral spine, merges into a single nerve in the pelvis, and runs down the back of the thigh, branching into the lower leg and foot.
When people say they have sciatica, they're describing that characteristic pattern of leg pain. What they're not specifying is where the problem originates, which nerve root is involved, or what's causing the irritation — all of which matter for treatment.
Why the term 'sciatica' is clinically limited
Sciatica describes symptoms. It doesn't specify:
• Which nerve root is affected (L4, L5, S1, or others)
• What's causing the irritation (disc herniation, stenosis, piriformis, other)
• Whether there is true nerve root compression or just nerve irritation
• The severity or prognosis of the condition
Two patients both describing 'sciatica' may have completely different underlying causes requiring different treatment approaches.
What Radiculopathy Means
Radiculopathy is the clinical term for a syndrome caused by dysfunction of a spinal nerve root. It can involve any combination of pain, numbness, tingling, and weakness in the distribution of that nerve root — a specific, predictable territory of the body called a dermatome.
Lumbar radiculopathy means the affected nerve root is in the lumbar spine. The symptoms travel into the leg. Cervical radiculopathy affects nerve roots in the neck and produces symptoms into the arm.
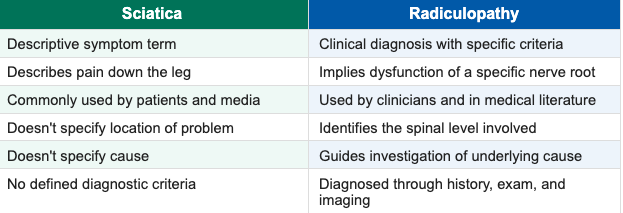
The key distinction from sciatica: radiculopathy is a clinical diagnosis with specific criteria. It implies a nerve root problem at a defined spinal level, with symptoms that follow the anatomical distribution of that root. It is more precise than sciatica and more directly guides treatment decisions.
What a 'Pinched Nerve' Actually Means
Pinched nerve is another lay term — even less precise than sciatica. It's used colloquially to describe any situation where a nerve is being compressed or irritated, producing symptoms along its path.
In clinical terms, true nerve root compression — where a structure like a herniated disc or bone spur is physically pressing on a nerve root — is one cause of radiculopathy. But nerve root irritation can also occur through inflammation, chemical irritation from disc material, or increased mechanosensitivity without significant structural compression.
This matters because the degree of structural compression on imaging doesn't always match the severity of symptoms. Some patients with large disc herniations have minimal symptoms. Others with modest compression have severe radiculopathy. The nerve's response to irritation is the variable — not just the compression itself.
How Clinicians Identify Which Nerve Root Is Involved
Each nerve root in the lumbar spine supplies a predictable region of skin (dermatome), muscle (myotome), and reflex. A skilled clinician uses the pattern of your symptoms — combined with physical examination — to identify which level is most likely responsible.
This is important because treatment, prognosis, and red flags differ by level. Here is the clinical map for the most commonly affected lumbar nerve roots:
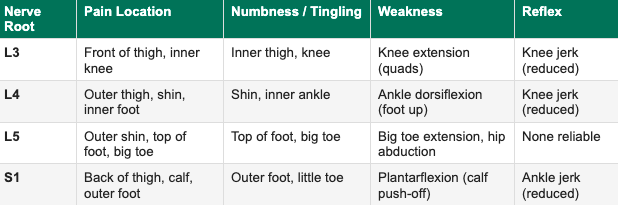
In practice, symptom patterns are often mixed or don't follow textbook distributions perfectly. Clinical examination — including muscle testing, reflex testing, and nerve tension tests like the straight leg raise — is used alongside imaging to build the full picture.
The straight leg raise test
One of the most commonly used tests for lumbar radiculopathy. With you lying on your back, your clinician lifts your leg with the knee straight. A positive test — reproduction of your leg pain (not just hamstring tightness) between 30 and 70 degrees — suggests nerve root tension, most commonly at L4, L5, or S1.
Sensitivity: approximately 80% (good at ruling out radiculopathy when negative)
Specificity: approximately 40% (less reliable at confirming it when positive)
Clinical examination findings are always interpreted alongside history and imaging — not in isolation.
The Most Common Causes of Lumbar Radiculopathy
Lumbar disc herniation
The most common cause in people under 50. When disc material herniates and contacts a nerve root, it causes both mechanical compression and a chemical inflammatory response. The inflammatory component is often the primary driver of acute radicular pain — which is why anti-inflammatory treatments can provide meaningful short-term relief.
See our full article on lumbar disc herniation for a detailed breakdown of what MRI findings mean and what natural history looks like.
Lumbar spinal stenosis
More common in people over 50. Stenosis refers to narrowing of the spinal canal or foraminal openings through which nerve roots exit. This narrowing — caused by bone spurs, thickened ligaments, or disc degeneration — can compress nerve roots, typically producing symptoms that worsen with standing and walking and improve with sitting or forward flexion. This pattern is called neurogenic claudication and is characteristic of stenotic radiculopathy.
Degenerative changes and foraminal narrowing
Age-related changes including bone spur formation (osteophytes) and disc height loss can gradually narrow the foramen through which a nerve root exits, causing chronic low-grade radiculopathy. This tends to produce more persistent, less acute symptoms than disc herniation.
Piriformis syndrome — a frequently misdiagnosed cause
The sciatic nerve passes either through or directly beneath the piriformis muscle in the buttock. In some people, tightness or hypertrophy of the piriformis can compress the sciatic nerve — producing symptoms that closely mimic lumbar radiculopathy but originate outside the spine entirely.
Distinguishing piriformis syndrome from true lumbar radiculopathy is clinically important because the treatment is completely different. Piriformis syndrome does not respond to spinal-focused treatment and instead requires targeted hip and piriformis rehabilitation.
Key differentiators: Piriformis syndrome typically produces buttock pain and posterior leg symptoms without clear dermatomal distribution, is reproduced by direct piriformis provocation tests, and is not associated with the spinal movement patterns that aggravate true radiculopathy.
Why the Distinction Matters for Treatment
This is the clinical payoff of the terminology. The specific cause and level of your radiculopathy should directly drive your treatment approach. Here is how the differentiation changes management:
Disc herniation at L4–L5 or L5–S1: Directional preference exercises (often extension-based), neural mobilization, progressive loading, activity modification. High rate of spontaneous resolution. Epidural steroid injection as a bridge if symptoms are severe.
Stenotic radiculopathy: Flexion-based exercises typically provide relief (the opposite of disc herniation). Aquatic therapy, stationary cycling, and positions that open the spinal canal are often effective. Stenosis does not spontaneously resolve the way disc herniation does — management is the goal, not cure.
Piriformis syndrome: Piriformis stretching, hip external rotator strengthening, soft tissue work to the piriformis and surrounding musculature. Spinal exercises are not the primary intervention.
Foraminal stenosis from degenerative changes: Traction-based techniques, neural mobilization, postural correction, and strengthening to reduce compressive forces on the foramen. Management of contributing factors like hip mobility and thoracic extension.
A treatment program built for disc herniation may be actively unhelpful for stenosis — and vice versa. This is a primary reason why generic back pain exercise programs frequently underperform individualized rehabilitation: they don't account for what's actually driving the symptoms.
What Treatment Has the Strongest Evidence
Physical therapy — individualized, not generic
The evidence for physical therapy in lumbar radiculopathy is strong, with the critical caveat that it must be individualized to the specific cause and presentation. A thorough evaluation that identifies the likely nerve root level, the probable cause, and the directional preference of the condition is the foundation of effective PT.
Key components of evidence-based PT for radiculopathy include neural mobilization, directional preference exercises, progressive spinal loading, and education about the neuroscience of nerve pain — which behaves differently from musculoskeletal pain and requires different patient expectations.
Pain management in the acute phase
Nerve root pain can be severe. Short-term use of NSAIDs, neuropathic pain medications (gabapentin, pregabalin), or oral corticosteroids may be appropriate in the acute phase to allow participation in rehabilitation. Epidural steroid injections can provide meaningful short-term relief for acute disc-related radiculopathy specifically.
Staying active within a tolerable range
As with low back pain generally, prolonged rest worsens outcomes for radiculopathy. Identifying positions and movements that are tolerable — and building from there — is consistently associated with better recovery than activity avoidance.
Time and natural history
The majority of lumbar radiculopathy caused by disc herniation resolves significantly within 6–12 weeks with conservative care, consistent with the spontaneous regression data discussed in our disc herniation article. Stenotic radiculopathy has a different natural history — it tends to be more persistent and requires ongoing management rather than expecting full resolution.
When Radiculopathy Requires Urgent Attention
Seek immediate medical evaluation for any of the following:
• Loss of bladder or bowel control alongside leg symptoms
• Numbness in the groin, inner thighs, or saddle area (perineum)
• Rapidly progressive leg weakness — strength declining over days
• Bilateral leg symptoms (both legs affected simultaneously)
• Back pain with fever, unexplained weight loss, or history of cancer
These symptoms may indicate cauda equina syndrome or another serious spinal condition requiring emergency evaluation. Do not wait.
Key Takeaways
• Sciatica is a symptom description — pain down the leg — not a diagnosis
• Radiculopathy is the clinical term for nerve root dysfunction, with specific patterns of pain, numbness, tingling, and weakness
• Identifying which nerve root is involved (L4, L5, S1, etc.) directly guides treatment
• The most common causes are disc herniation (under 50) and spinal stenosis (over 50), which require opposite treatment approaches
• Piriformis syndrome mimics lumbar radiculopathy but originates in the hip — and is frequently misdiagnosed
• Effective physical therapy for radiculopathy is individualized to the specific cause — generic exercise programs often underperform
• Most disc-related radiculopathy resolves within 6–12 weeks with conservative care; stenotic radiculopathy requires longer-term management
• Loss of bladder/bowel control or rapidly progressive leg weakness require immediate emergency evaluation
Frequently Asked Questions
Is sciatica the same as radiculopathy?
Sciatica and radiculopathy overlap but aren't identical. Sciatica describes pain traveling down the back of the leg via the sciatic nerve distribution. Radiculopathy is the broader clinical term for any nerve root dysfunction — which can produce pain, numbness, tingling, or weakness in the distribution of a specific nerve root. All sciatica involves some form of radiculopathy, but not all radiculopathy produces classic sciatica symptoms.
How do I know if my leg pain is sciatica or something else?
True sciatica or lumbar radiculopathy typically follows a specific path — often from the buttock down the back of the thigh, into the calf, and potentially into the foot. It may worsen with sitting, bending forward, or coughing. General leg pain that doesn't follow a dermatomal pattern, or pain that's primarily in the knee or hip, is less likely to be radiculopathy. A clinical evaluation is the most reliable way to differentiate — imaging alone is insufficient.
Can sciatica go away on its own?
Yes, and frequently does. When caused by lumbar disc herniation — the most common cause — most cases of sciatica resolve significantly within 6–12 weeks with conservative care, consistent with the high rate of spontaneous disc regression. Sciatica from stenosis is less likely to fully resolve but can often be effectively managed. Early, appropriate physical therapy shortens recovery time and reduces recurrence risk.
What is the fastest way to relieve sciatic nerve pain?
There is no reliable shortcut, but several approaches consistently help in the acute phase: identifying positions of relief (often lying with the knee supported in extension for disc-related sciatica), gentle neural mobilization exercises, short-term anti-inflammatory medication if tolerated, and staying as active as symptoms allow. A physical therapist can identify your directional preference — the specific movement pattern that centralizes your symptoms — which is often the single most impactful early intervention.
Can sitting cause sciatica?
Prolonged sitting increases intradiscal pressure and can aggravate disc-related radiculopathy, but sitting itself doesn't cause structural nerve damage. If your symptoms consistently worsen with sitting, this suggests a disc herniation is a likely driver — flexion-intolerant presentations typically respond well to extension-based exercises. If sitting relieves your symptoms and walking worsens them, stenosis is a more likely cause.
Do I need an MRI to diagnose sciatica?
Not necessarily for initial management. A thorough clinical history and physical examination — including dermatomal testing, reflex testing, muscle strength testing, and nerve tension tests — can identify the likely nerve root involved and guide initial treatment. MRI is indicated when symptoms are severe or progressive, when surgery is being considered, when red flag symptoms are present, or when symptoms fail to improve with appropriate conservative care.
Dealing with leg pain, numbness, or sciatica?
Book a free 15-minute discovery call with us today. We'll talk through your symptoms, what's likely driving them, and whether a telehealth rehab program is the right next step.
spine33rehab.com | Book Your Free Call
About the Author
Dr. Connor Sheeks PT, DPT is a licensed physical therapist and the founder of Spine 33 Rehab PLLC, a cash-pay telehealth physical therapy practice specializing in virtual spine rehabilitation. He holds a Doctor of Physical Therapy (DPT) degree and has clinical experience treating chronic low back pain, lumbar disc herniation and radiculopathy, cervicogenic headache, lumbar spinal stenosis, postural dysfunction, and many other spinal pathologies. Spine33 Rehab currently serves patients in Tennessee via telehealth and is actively pursuing licenses in other states.
References
Konstantinou K, Dunn KM. (2008). Sciatica: review of epidemiological studies and prevalence estimates. Spine. doi:10.1097/BRS.0b013e318183a4a5
Ropper AH, Zafonte RD. (2015). Sciatica. New England Journal of Medicine. doi:10.1056/NEJMra1410151
Deyo RA, Mirza SK. (2016). Herniated lumbar intervertebral disk. New England Journal of Medicine. doi:10.1056/NEJMcp1512658
Fairbank J, et al. (2011). Randomised controlled trial to compare surgical stabilisation of the lumbar spine with an intensive rehabilitation programme for patients with chronic low back pain. BMJ. doi:10.1136/bmj.d2495
Boyajian-O'Neill LA, et al. (2008). Diagnosis and management of piriformis syndrome: an osteopathic approach. Journal of the American Osteopathic Association.
Iversen T, et al. (2011). Accuracy of physical examination for chronic lumbar radiculopathy. BMC Musculoskeletal Disorders. doi:10.1186/1471-2474-12-207