
Neck Pain and Headaches: Why Your Headaches Might Actually Be A Spine Problem
Written by Connor Sheeks PT, DPT · Published May 2026 · Last reviewed May 2026
Reading time: approximately 9 minutes

If you've had recurring headaches for months or years — headaches that start at the base of your skull, travel over one side of your head, and seem to be connected to your neck — there's a real chance they've been misdiagnosed.
Cervicogenic headache is a type of headache that originates from the cervical spine — the joints, muscles, and nerves of the neck — and refers pain into the head. It accounts for an estimated 15–20% of all chronic recurring headaches. And because its symptoms can overlap significantly with tension headache and migraine, it is frequently missed, undertreated, or treated with approaches that don't address the source.
The clinical implication is significant: if your headaches are cervicogenic in origin, no amount of migraine medication or tension headache management will produce lasting relief. The neck needs to be treated. And that's exactly what physical therapy — specifically, manual therapy and targeted exercise for the cervical spine — is designed to do.
This article explains what cervicogenic headache is, how to distinguish it from other headache types, what the cervical spine has to do with it, and what treatment actually works.
What you'll learn in this article
• What cervicogenic headache is and where it comes from anatomically
• How to distinguish it from tension headache and migraine
• The cervical spine structures most commonly involved
• Why it's frequently misdiagnosed and undertreated
• What physical therapy does for cervicogenic headache — and what the evidence shows
• What a realistic treatment plan and recovery timeline looks like
• When headaches require urgent medical evaluation
What Cervicogenic Headache Is
Cervicogenic headache (CGH) is a headache that originates from a source in the cervical spine — typically the upper cervical joints (C1–C3), surrounding musculature, or the suboccipital region — and refers pain into the head through shared neural pathways.
The anatomical basis for this is well established. The upper cervical nerve roots (C1, C2, C3) converge with the trigeminal nerve — the primary sensory nerve of the face and head — in a region of the brainstem called the trigeminal cervical nucleus. This convergence means that pain signals originating in the neck can be perceived as headache pain in the forehead, temples, eye, or top of the head.
In plain terms: your brain can misidentify the source of the pain signal. The neck is the generator, but the head is where you feel it.
The trigeminocervical nucleus — why neck problems cause head pain
Pain signals from the upper cervical spine (C1–C3) and from the face/head (via the trigeminal nerve) converge in the same region of the brainstem.
This convergence means the brain cannot always distinguish between a pain signal coming from the neck versus one coming from the head — so neck-sourced pain is frequently perceived as headache.
This is the same mechanism that causes referred pain in other parts of the body — like how a heart attack can cause left arm pain. The source and the perceived location are different.
Cervicogenic Headache vs. Tension Headache vs. Migraine
These three headache types share overlapping features, which is why misdiagnosis is common. The distinctions matter because they point to different treatment targets.
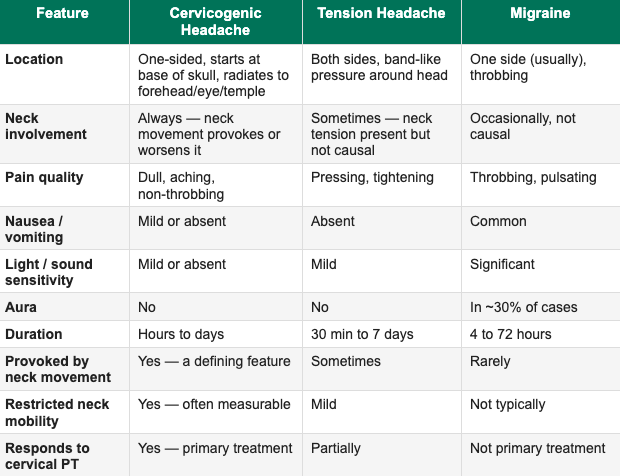
The most reliable distinguishing feature of cervicogenic headache is that neck movement — rotation, extension, or sustained postures — consistently provokes or worsens the headache. This is a defining diagnostic criterion. If turning your head, looking up, or sitting at a desk for extended periods reliably triggers your headache, the cervical spine is likely involved.
Which Cervical Structures Are Most Commonly Involved
Not all neck structures contribute equally to cervicogenic headache. Research and clinical experience consistently point to the upper cervical region as the primary source:
The upper cervical joints — C1/C2 and C2/C3
The zygapophyseal (facet) joints at C1/C2 and C2/C3 are the most commonly identified pain sources in cervicogenic headache. These joints are richly innervated and lie in close proximity to the nerve roots that feed into the trigeminocervical nucleus. Joint dysfunction — restricted mobility, inflammation, or altered mechanics at these levels — is the structural driver in most CGH cases.
A diagnostic nerve block at the C2/C3 facet joint is considered the gold standard for confirming cervicogenic headache — if blocking that joint eliminates the headache, the diagnosis is confirmed. In clinical PT practice, manual examination of upper cervical joint mobility is the primary assessment tool.
The suboccipital musculature
The suboccipital muscles — a group of four small muscles at the base of the skull connecting C1 and C2 to the occiput — are frequently hypertonic (chronically overactive) in cervicogenic headache. Their proximity to the C2 nerve root means that sustained tension or trigger points in this region can directly provoke headache symptoms.
Prolonged forward head posture, screen time, and sustained cervical flexion all load the suboccipital muscles heavily — which is why cervicogenic headache is increasingly common in desk workers and people with high screen exposure.
The cervical deep flexors
The deep cervical flexor muscles — longus colli and longus capitis — are the primary stabilizers of the cervical spine. Research consistently shows that people with chronic neck pain and cervicogenic headache have measurably impaired deep cervical flexor endurance and neuromuscular control. This loss of stability places additional mechanical stress on the upper cervical joints and surrounding structures, perpetuating the headache cycle.
Restoring deep cervical flexor function is a core component of effective Physical Therapy for cervicogenic headache — and one of the primary reasons it works.
Why Cervicogenic Headache Is Frequently Misdiagnosed
Several factors contribute to the high misdiagnosis rate:
Symptom overlap with migraine. CGH can produce unilateral head pain, light sensitivity, and nausea — features commonly associated with migraine. Without a careful history focused on neck provocation and a manual cervical assessment, the distinction is easy to miss.
Most headache evaluations don't include cervical examination. A standard neurology or primary care evaluation for headache typically involves history, neurological screening, and possibly neuroimaging. Hands-on assessment of cervical joint mobility and upper cervical tenderness is not standard in non-PT settings.
Patients don't connect their neck to their headache. Most people with CGH report neck pain and headaches as separate problems. The connection — that the neck is generating the headache — is rarely intuitive without clinical explanation.
Partial medication response creates diagnostic confusion. Triptans and other migraine medications sometimes provide partial relief for CGH, which can reinforce an incorrect diagnosis and delay appropriate treatment.
What Physical Therapy Does for Cervicogenic Headache
Physical therapy is the most evidence-supported primary treatment for cervicogenic headache. A 2012 Cochrane Review and multiple subsequent randomized controlled trials consistently show that manual therapy combined with specific exercise produces meaningful, lasting reduction in headache frequency, intensity, and duration.
Here is what an effective PT program for CGH actually involves:
Manual therapy to the upper cervical spine
Hands-on assessment and treatment of C1/C2 and C2/C3 joint mobility is the foundation. Techniques include joint mobilization — gentle, graded movement applied to restricted segments — and, where appropriate, high-velocity manipulation. Research shows that upper cervical mobilization produces immediate and sustained reduction in headache intensity for most CGH patients.
This is one component of treatment that requires hands-on care — it cannot be fully replicated through exercise alone, which is why a provider with manual therapy training is important for this condition specifically.
Deep cervical flexor retraining
Craniocrervical flexion training — a specific protocol for restoring neuromuscular control of the deep cervical flexors — has a strong evidence base for cervicogenic headache. It involves graduated activation of the deep stabilizers through precise, low-load movements that most patients have never performed correctly. It is not a generic 'chin tuck' exercise. The progression is specific, measured, and takes several weeks.
Postural correction and load management
Sustained forward head posture places significant mechanical load on the upper cervical spine. For every inch the head translates forward from its neutral position over the shoulders, the effective weight on the cervical spine increases by approximately 10 pounds. Correcting this pattern — through awareness, workstation modification, and strengthening the posterior cervical and thoracic musculature — reduces the structural load that perpetuates CGH.
Suboccipital soft tissue work
Direct treatment of the suboccipital muscles — through sustained pressure, muscle energy techniques, or targeted stretching — can reduce the local muscle tension contributing to headache provocation. This is typically combined with joint mobilization rather than used in isolation.
Thoracic spine mobilization
Research shows that thoracic spine mobilization — treatment applied to the mid-back — produces measurable improvements in cervical range of motion and reduces cervicogenic headache frequency. This is likely because thoracic mobility restrictions directly affect the mechanics of the upper cervical spine. Treating only the neck without addressing thoracic mobility frequently produces incomplete results.
What the evidence shows — CGH outcomes with PT
A landmark 2002 RCT by Jull et al. (considered the defining study in cervicogenic headache PT research) found:
• Manual therapy alone: 68% reduction in headache frequency
• Exercise alone: 58% reduction in headache frequency
• Combined manual therapy + exercise: 76% reduction in headache frequency
• Control group: no meaningful change
Effects were maintained at 12-month follow-up. Combined treatment produced the strongest and most durable outcomes.
What a Realistic Treatment Plan Looks Like
A well-designed PT program for cervicogenic headache typically follows this general arc:
Weeks 1–2: Comprehensive cervical assessment, identification of primary pain generators (upper cervical joints, suboccipital region, thoracic mobility), manual therapy to restricted segments, introduction of deep cervical flexor training at low load, postural awareness.
Weeks 3–4: Progression of manual therapy intensity, advancement of deep flexor training, addition of thoracic mobilization, introduction of cervical strengthening in supported positions, workstation and posture modification plan.
Weeks 5–8: Most patients see meaningful reduction in headache frequency and intensity by this point. Progression toward unsupported strengthening, endurance training, and load tolerance. Manual therapy frequency typically reduces as active exercise takes over.
Weeks 8–12: Consolidation of gains, transition to independent home program, education on self-management of flare-ups, long-term maintenance strategy.
Most patients with cervicogenic headache see meaningful improvement within 6–8 weeks of consistent treatment. Patients with longer symptom histories or significant postural contributors may take 10–12 weeks for full benefit.
An important distinction from migraine management: the goal of CGH treatment is not just reduction of individual headache episodes. It is correction of the underlying cervical dysfunction that generates them. Done well, Physical Therapy produces durable change — not indefinite management.
Can Telehealth PT Effectively Treat Cervicogenic Headache?
This is a legitimate question given that manual therapy — hands-on joint mobilization — is a core component of CGH treatment. Here is an honest answer:
The manual therapy component of cervicogenic headache treatment does require in-person care for best results. Joint mobilization of the upper cervical spine cannot be fully replicated via video.
However, a significant portion of effective CGH treatment is fully deliverable via telehealth:
Deep cervical flexor retraining — all of this is exercise-based and coaches well over video
Postural correction and workstation assessment — telehealth is actually advantageous here, since your therapist can see your actual environment
Thoracic mobility exercises — fully deliverable remotely
Cervical strengthening and endurance training — fully deliverable remotely
Education on self-management, trigger identification, and flare-up response — fully deliverable remotely
Self-mobilization techniques — specific self-treatment strategies can be taught and coached via video
For patients who have already had a manual therapy course from an in-person provider and need ongoing rehab and maintenance, telehealth PT is highly appropriate. For patients who have not yet had upper cervical manual therapy and whose headaches are primarily driven by joint restriction, a hybrid approach — or referral to a local manual therapy provider in conjunction with telehealth programming — may produce the best outcome.
At Spine33 Rehab, we will tell you honestly at your discovery call which approach is the right fit for your presentation. We will not take on a case where in-person care is clearly the superior option without having that conversation first.
When Headaches Require Urgent Medical Evaluation
Seek immediate medical attention for any of the following:
• Sudden, severe headache unlike any you've had before ('thunderclap headache')
• Headache with fever, stiff neck, and sensitivity to light — possible meningitis
• Headache with neurological symptoms: vision changes, slurred speech, facial drooping, arm weakness
• Headache following head or neck trauma
• Headache that wakes you from sleep and progressively worsens
• New headache pattern in someone over 50 years old with no prior headache history
• Headache with unexplained weight loss or history of cancer
These are red flags for serious intracranial conditions requiring emergency evaluation.
Key Takeaways
• Cervicogenic headache originates from structures in the cervical spine — usually the upper cervical joints (C1–C3) — and refers pain into the head through shared neural pathways
• It accounts for an estimated 15–20% of all chronic recurring headaches and is frequently misdiagnosed as migraine or tension headache
• The defining clinical feature: neck movement consistently provokes or worsens the headache
• The upper cervical joints (C1/C2, C2/C3), suboccipital musculature, and deep cervical flexors are the primary structures involved
• Physical therapy — combining upper cervical manual therapy with specific exercise — is the most evidence-supported treatment and produces durable outcomes
• Combined manual therapy plus exercise reduces headache frequency by up to 76% in clinical trials, with effects maintained at 12 months
• Telehealth PT is appropriate for most of the exercise and rehabilitation components; some patients benefit from an in-person manual therapy component as well
• Sudden severe headache, neurological symptoms, or headache with fever require emergency evaluation
Frequently Asked Questions
How do I know if my headaches are cervicogenic or something else?
The most reliable indicator is whether neck movement, sustained neck postures, or pressure on the upper neck consistently provokes your headache. Cervicogenic headache is also typically one-sided, starts at the base of the skull and radiates forward, and is associated with restricted neck mobility. A physical therapist with training in cervical assessment can evaluate your upper cervical joints and determine whether they are the likely source. Neuroimaging rules out serious causes but does not diagnose CGH — clinical examination does.
Can a physical therapist help with headaches?
Yes — specifically for cervicogenic headache, physical therapy is the primary evidence-based treatment. Manual therapy to the upper cervical spine combined with specific exercise produces meaningful, lasting reductions in headache frequency and intensity. PT is not the primary treatment for classic migraine (which requires neurological management) but is an effective adjunct for cervical contributors in mixed presentations.
What does cervicogenic headache feel like?
Typically: a dull, aching pain that starts at the base of the skull or upper neck on one side, radiates forward over the top of the head toward the forehead, temple, or eye. It may feel like pressure behind the eye. It is usually not throbbing. It is often accompanied by neck stiffness and may be worsened by sustained postures, looking up, or rotating the head. Nausea and light sensitivity can occur but are typically mild.
What is the best treatment for cervicogenic headache?
The strongest evidence supports a combination of upper cervical manual therapy and specific therapeutic exercise — specifically deep cervical flexor retraining. This combined approach produces significantly better outcomes than either treatment alone. A thorough cervical assessment to identify the specific joints and structures involved should precede any treatment plan.
Can forward head posture cause headaches?
Yes, and this is one of the most common contributing factors to cervicogenic headache — particularly in people with high screen exposure or desk-based work. Forward head posture significantly increases the mechanical load on the upper cervical spine and chronically overloads the suboccipital musculature. Correcting this pattern through postural retraining, workstation modification, and cervical strengthening is a core part of effective CGH management.
How long does it take for physical therapy to help cervicogenic headaches?
Most patients see meaningful reduction in headache frequency and intensity within 6–8 weeks of consistent treatment. Some notice improvement within the first two to three sessions following upper cervical manual therapy. Full benefit — including durable, independent management — typically takes 10–12 weeks for a complete course of care.
Have headaches that no one has been able to explain?
Book a free 15-minute discovery call with us today. We'll talk through your symptom pattern, what's likely driving it, and whether cervicogenic headache treatment is the right fit for you.
spine33rehab.com | Book Your Free Call
About the Author
Dr. Connor Sheeks PT, DPT is a licensed physical therapist and the founder of Spine 33 Rehab PLLC, a cash-pay telehealth physical therapy practice specializing in virtual spine rehabilitation. He holds a Doctor of Physical Therapy (DPT) degree and has clinical experience treating chronic low back pain, lumbar disc herniation and radiculopathy, cervicogenic headache, lumbar spinal stenosis, postural dysfunction, and many other spinal pathologies. Spine33 Rehab currently serves patients in Tennessee via telehealth and is actively pursuing licenses in other states.
References
Jull G, et al. (2002). A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache. Spine. doi:10.1097/00007632-200210010-00004
Sjaastad O, Fredriksen TA, Pfaffenrath V. (1998). Cervicogenic headache: diagnostic criteria. Headache. doi:10.1046/j.1526-4610.1998.3808442.x
Bogduk N, Govind J. (2009). Cervicogenic headache: an assessment of the evidence on clinical diagnosis, invasive tests, and treatment. Lancet Neurology. doi:10.1016/S1474-4422(09)70209-1
Niere K, Jerak A. (2004). Measurement of headache frequency, intensity and duration: comparison of patient report by questionnaire and headache diary. Physiotherapy Research International.
Gross A, et al. (2015). Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD004249.pub4
Falla DL, Jull GA, Hodges PW. (2004). Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexion test. Spine. doi:10.1097/01.brs.0000146464.40684.7f