
Lumbar Disc Herniation: What Your MRI Actually Means (And Why It Matters Less Than You Think)
Written by Connor Sheeks PT, DPT · Published April 2026 · Last reviewed May 2026
Reading time: approximately 9 minutes

You got your MRI results back. The report uses words like disc herniation, annular tear, nerve impingement, or foraminal narrowing. Your doctor said something about it, maybe briefly, and now you're sitting with a piece of paper that sounds alarming and a lot of unanswered questions.
What does this actually mean for your spine? How did this happen? Does it mean you need surgery? Is this permanent? Are you going to get worse?
These are the right questions. And the answers are probably not what you've been told — or what you've assumed based on the language in that report.
This article is a plain-language breakdown of what lumbar disc herniation actually is, what MRI findings do and don't tell us, what the research shows about outcomes, and what actually helps.
What you'll learn in this article
• What a lumbar disc herniation actually is — in plain language
• Why MRI findings are a poor predictor of pain and disability
• The difference between a disc herniation and radiculopathy (sciatica)
• What the natural history of disc herniation looks like without surgery
• What treatment options actually have evidence behind them
• When surgery is and isn't appropriate
• What recovery realistically looks like
What a Lumbar Disc Herniation Actually Is
Your lumbar spine has five vertebrae (L1 through L5) stacked on top of each other, with a rubbery disc between each pair. Each disc has two parts: a tough outer ring called the annulus fibrosus, and a softer gel-like center called the nucleus pulposus.
A disc herniation occurs when the soft inner material pushes through a weakness or tear in the outer ring. Depending on how far it pushes through and in what direction, it may or may not contact nearby nerve tissue.
MRI reports use several terms for this, and they are not all the same thing:
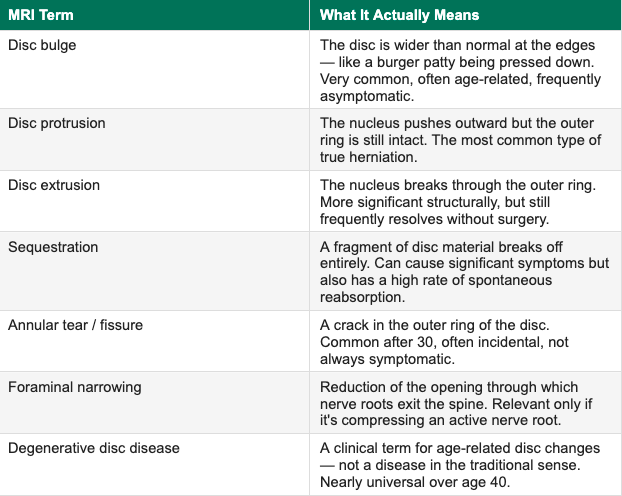
The key point: these are anatomical descriptions, not diagnoses. Finding them on an MRI tells you what the tissue looks like. It does not tell you whether that finding is causing your symptoms.
Why Your MRI Findings May Not Explain Your Pain
This is the part that surprises most people — and that most patients are never told directly.
In 2015, a systematic review published in the American Journal of Neuroradiology pooled data from 33 studies and examined MRI findings in people with no back pain whatsoever. The results were striking:
MRI findings in people with NO back pain (Brinjikji et al., 2015)
• Age 20: 37% had disc degeneration | 30% had disc bulges | 29% had disc height loss
• Age 40: 68% had disc degeneration | 50% had disc bulges | 45% had disc height loss
• Age 60: 91% had disc degeneration | 71% had disc bulges | 62% had disc height loss
• Age 80: 96% had disc degeneration | 84% had disc bulges
These findings were present with zero symptoms. They are part of normal spinal aging.
What this means practically: when your MRI report lists disc bulges or degeneration, it is very likely describing the normal aging process of your spine — not a structural explanation for your pain.
This does not mean disc herniations never cause symptoms. They do. When a herniated disc contacts and irritates a nerve root, it can cause genuine radicular symptoms — pain, numbness, tingling, or weakness that radiates down the leg in a predictable pattern. That is a real, clinically significant finding.
But a disc herniation on MRI without corresponding nerve symptoms is a much weaker explanation for back pain than most patients are led to believe. And treating an asymptomatic or mildly symptomatic finding aggressively — with injections, procedures, or surgery — frequently makes outcomes worse.
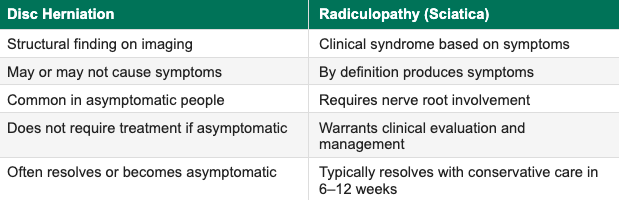
Disc Herniation vs. Radiculopathy: What's the Difference?
These terms are often used interchangeably, but they describe different things.
Disc herniation is the structural finding — a disc pushing beyond its normal boundary, visible on MRI.
Radiculopathy is the clinical syndrome — symptoms caused by irritation or compression of a nerve root, including pain, numbness, tingling, or weakness radiating down the arm or leg in a specific pattern.
You can have a disc herniation without radiculopathy. You can also have radiculopathy without a clearly visible herniation on MRI. The clinical picture — your symptoms, their distribution, and how they behave — matters more than the imaging alone.
Sciatica is a common term for lumbar radiculopathy — specifically pain that radiates down the back of the leg, often into the calf or foot, caused by irritation of the sciatic nerve or its contributing nerve roots (typically L4, L5, or S1).
What Happens to a Disc Herniation Without Surgery?
This is the most important thing most patients are never told: disc herniations have a high rate of spontaneous regression — meaning they shrink and often disappear on their own, without any intervention.
A 2017 systematic review in the American Journal of Neuroradiology examined rates of spontaneous regression across multiple studies. The findings:
Disc protrusions: 41% showed regression, 15% completely resolved
Disc extrusions (the more severe type): 96% showed some regression, 43% completely reabsorbed
Sequestrated fragments (the most severe type): showed the highest rate of reabsorption — over 96%
The biology behind this is well understood: the immune system recognizes extruded disc material as foreign tissue and actively works to reabsorb it. The more material that has extruded, the more aggressively this process tends to occur — which is why the most severe herniations often have the best natural history.
This has direct implications for treatment decisions. Many patients are evaluated for surgery or aggressive intervention in the acute phase — when the disc herniation is at its largest and symptoms are worst. In most cases, waiting and pursuing conservative treatment during this window produces equivalent or better long-term outcomes.
What Treatment Options Actually Have Evidence Behind Them
Physical therapy — first-line treatment
Physical therapy is the most evidence-supported first-line treatment for symptomatic lumbar disc herniation. A comprehensive PT program addresses multiple drivers simultaneously: nerve mobility, movement patterning, progressive spinal loading, and the fear-avoidance that often develops around radicular symptoms.
Specific approaches with strong evidence for disc herniation and radiculopathy include:
Directional preference exercises (McKenzie Method) — identifying positions and movements that centralize symptoms, meaning they move pain from the leg toward the spine, which is a positive prognostic sign
Neural mobilization — gentle techniques to restore mobility of the nerve root and reduce mechanosensitivity
Progressive loading — systematic strengthening of the lumbar spine, hips, and posterior chain to reduce compressive demands on the disc
Education and activity modification — understanding which positions and activities to temporarily avoid versus which are safe and beneficial
Activity modification — not rest
As with chronic low back pain generally, prolonged rest is not recommended for disc herniation. Staying active within a comfortable range, avoiding provocative positions, and gradually expanding activity is consistently associated with better outcomes than bed rest.
Pain management in the acute phase
Short-term use of anti-inflammatory medications (NSAIDs) can help manage acute radicular pain enough to allow participation in rehab. Epidural steroid injections can provide short-term relief for severe radicular symptoms — not as a cure, but as a bridge that allows a patient to engage with physical therapy. The evidence does not support injections as a standalone long-term treatment.
Time
Given the high rate of spontaneous regression, time is genuinely one of the most important variables for disc herniation recovery. The majority of patients with symptomatic lumbar disc herniation improve significantly within 6–12 weeks with conservative care. This is not passive waiting — it is active rehab during a period when the natural history is working in your favor.
When Is Surgery Actually Appropriate?
Surgery for lumbar disc herniation is appropriate in a minority of cases. The clearest indications are:
Cauda equina syndrome — loss of bladder or bowel control, numbness in the saddle area (groin and inner thighs), or progressive bilateral leg weakness. This is a surgical emergency requiring immediate evaluation.
Progressive neurological deficit — leg weakness that is worsening over days to weeks despite conservative care
Severe, unremitting radiculopathy that has not responded to 6–12 weeks of quality conservative treatment
Surgery is generally not indicated for back pain alone without significant nerve symptoms, for MRI findings without corresponding clinical symptoms, or as a first-line treatment before exhausting conservative care.
When surgery is indicated, microdiscectomy — a minimally invasive procedure to remove the portion of disc pressing on the nerve — has good outcomes for radiculopathy specifically. It typically produces faster relief of leg symptoms than conservative care in patients who meet the criteria above. What it does not do is prevent future disc problems or address the underlying factors that contributed to the herniation.
Seek immediate medical attention if you experience:
• Loss of bladder or bowel control
• Numbness or tingling in the groin, inner thighs, or saddle area
• Rapidly progressing leg weakness
• Back pain with fever
These symptoms may indicate cauda equina syndrome, a medical emergency.
What Recovery Actually Looks Like
Recovery from lumbar disc herniation is rarely linear. Here is an honest timeline for most patients undergoing conservative care:
Weeks 1–3: Often the most difficult phase. Pain may be severe, radicular symptoms pronounced. Goals are pain management, identifying positions of relief, beginning gentle neural mobility work, and avoiding provocative loading.
Weeks 3–6: Most patients begin to notice centralization — leg symptoms retreating toward the back. This is a significant positive sign. Activity tolerance typically begins to improve. Physical Therapy program advances toward more active loading.
Weeks 6–12: The majority of patients with acute disc herniation see substantial improvement in this window. Full resolution of leg symptoms is common. Return to most activities, including exercise, is the target.
Months 3–6: Ongoing strengthening and progressive loading to restore full function and reduce recurrence risk. Some patients with larger herniations or chronic presentations take longer.
Beyond 6 months: Maintenance of a consistent movement and loading practice. The disc itself may take up to 12–18 months to fully reabsorb in extrusion cases, but functional recovery typically precedes full structural resolution.
A few things that genuinely affect recovery speed:
How long symptoms were present before starting rehab
How much fear-avoidance has developed around movement
Sleep quality, stress levels, and how consistently the exercise program is followed
None of these are fixed — all of them are addressable.
Key Takeaways
• A disc herniation is a structural finding — its presence on MRI does not automatically explain your pain
• MRI findings including disc bulges, degeneration, and even herniations are extremely common in people with no symptoms at all
• Disc herniation and radiculopathy (sciatica) are different things — radiculopathy requires nerve root involvement and specific symptom patterns
• The majority of disc herniations spontaneously regress over time — the most severe extrusions have the highest reabsorption rates
• Physical therapy is the evidence-supported first-line treatment for symptomatic disc herniation
• Surgery is appropriate for cauda equina syndrome, progressive neurological deficit, or severe radiculopathy unresponsive to conservative care — not for MRI findings alone
• Most patients with acute symptomatic disc herniation improve significantly within 6–12 weeks of quality conservative care
Frequently Asked Questions
Can a herniated disc heal on its own?
Yes — and frequently does. Research shows that disc herniations, including significant extrusions, have a high rate of spontaneous regression over months. The immune system actively reabsorbs extruded disc material. Most patients with acute symptomatic disc herniation improve substantially with conservative care within 6–12 weeks, without surgery.
How do I know if my back pain is from a disc herniation or something else?
A disc herniation causing nerve involvement typically produces radicular symptoms — pain, numbness, tingling, or weakness that radiates into the leg in a specific pattern (often below the knee), and may be worsened by sitting, forward bending, or Valsalva maneuvers like coughing. Back pain alone without leg symptoms is less likely to be driven primarily by nerve compression from a disc. A thorough clinical evaluation is more informative than MRI alone.
Is it safe to exercise with a herniated disc?
For most people, yes — with appropriate guidance. The goal of rehab is not to rest the disc but to restore movement, reduce nerve sensitization, and progressively load the spine. Certain positions and movements may be temporarily provocative and are modified in the early phases. A physical therapist can identify what is and isn't appropriate for your specific presentation.
Should I get surgery for my herniated disc?
Surgery is indicated for a minority of patients — those with cauda equina syndrome (a medical emergency), progressive leg weakness, or severe radiculopathy that hasn't responded to 6–12 weeks of quality conservative care. For most patients, surgery does not produce better long-term outcomes than conservative treatment and carries real risks. If surgery has been recommended, it is reasonable to pursue a thorough course of Physical Therapy first.
How long does it take to recover from a herniated disc?
Most patients with acute symptomatic herniation see meaningful improvement within 6–12 weeks of conservative care. Full resolution of symptoms can take 3–6 months. Some patients with larger herniations or longer symptom duration take up to 12 months for complete recovery. Structural reabsorption of extruded material can continue for up to 12–18 months.
My MRI shows multiple disc herniations. Is that worse?
Not necessarily. Multiple findings on MRI are common and frequently reflect normal age-related changes across multiple levels rather than a more serious condition. What matters clinically is whether any of those findings are producing nerve symptoms, and which level is most likely responsible. A thorough physical examination often tells us more than the number of findings on imaging.
Got a disc herniation diagnosis and not sure what to do next?
Book a free 15-minute discovery call with us today. We'll talk through your imaging, your symptoms, and whether a telehealth rehab program is the right next step.
spine33rehab.com | Book Your Free Call
About the Author
Dr. Connor Sheeks PT, DPT is a licensed physical therapist and the founder of Spine 33 Rehab PLLC, a cash-pay telehealth physical therapy practice specializing in virtual spine rehabilitation. He holds a Doctor of Physical Therapy (DPT) degree and has clinical experience treating chronic low back pain, lumbar disc herniation and radiculopathy, cervicogenic headache, lumbar spinal stenosis, postural dysfunction, and many other spinal pathologies. Spine33 Rehab currently serves patients in Tennessee via telehealth and is actively pursuing licenses in other states.
References
Brinjikji W, et al. (2015). Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR American Journal of Neuroradiology. doi:10.3174/ajnr.A4173
Chiu CC, et al. (2015). The probability of spontaneous regression of lumbar herniated disc: a systematic review. Clinical Rehabilitation. doi:10.1177/0269215514540919
Pinto RZ, et al. (2012). Epidural corticosteroid injections in the management of sciatica: a systematic review and meta-analysis. Annals of Internal Medicine. doi:10.7326/0003-4819-157-12-201212180-00008
Deyo RA, Mirza SK. (2016). Herniated lumbar intervertebral disk. New England Journal of Medicine. doi:10.1056/NEJMcp1512658
Konstantinou K, Dunn KM. (2008). Sciatica: review of epidemiological studies and prevalence estimates. Spine. doi:10.1097/BRS.0b013e318183a4a5