
Physical Therapy vs. Chiropractic for Back Pain: An Honest Comparison
Written by Connor Sheeks PT, DPT · Published June 2026 · Last reviewed June 2026
Reading time: approximately 7 minutes

If you have back pain and you are trying to figure out who to see, the physical therapy vs. chiropractic question comes up fast. Both claim to treat back pain. Both are widely available. Both have patients who swear by them.
What most comparison articles will not tell you is that this is not really a competition. The two professions have meaningfully different training, different treatment philosophies, and different evidence bases. Which one is right for you depends on what is driving your pain, what you are trying to accomplish, and what kind of care model you want.
This article gives you a straightforward comparison of both. We are a physical therapy practice, so we have a perspective. We have also tried to make this accurate enough that a chiropractor would not find much to argue with.
What you will learn in this article
• What physical therapists and chiropractors are actually trained to do
• How the treatment approaches differ in practice
• What the evidence shows for each in back pain specifically
• Where each approach tends to work best
• How to decide which is right for your situation
The Training Difference
Physical therapists complete a Doctor of Physical Therapy degree, a three-year postgraduate clinical doctorate following a bachelor's degree. Training covers musculoskeletal evaluation, neuroscience, exercise prescription, manual therapy, and rehabilitation across the lifespan. Licensure requires passing national and state board examinations.
Chiropractors complete a Doctor of Chiropractic degree, also a postgraduate program typically four years in length. Training focuses heavily on spinal assessment, spinal manipulation (adjustment), and the relationship between spinal structure and nervous system function. Licensure similarly requires board examinations.
Both are doctoral-level providers. The meaningful difference is emphasis: PT training centers on movement, exercise, and rehabilitation. Chiropractic training centers on spinal manipulation and structural alignment. Some chiropractors have additional training in rehabilitation exercise, and some physical therapists have advanced training in manual therapy and manipulation. But the core orientation of each profession differs, and that shapes how they approach back pain.
How the Treatment Approaches Differ
What a physical therapist does
A PT evaluation typically includes a detailed movement assessment, identification of contributing factors like strength deficits, mobility restrictions, or fear-avoidance patterns, and development of an individualized exercise and rehabilitation program. Treatment is primarily active, meaning the patient does the work, with manual therapy used as an adjunct to facilitate better movement or reduce pain enough to engage with exercise.
The explicit goal of PT is to make you less dependent on treatment over time, not more. A good PT program gives you tools and builds capacity so that you can manage your own spine health independently.
What a chiropractor does
A chiropractic visit typically centers on spinal manipulation, commonly called an adjustment, in which the chiropractor applies a controlled force to specific spinal segments to restore mobility, reduce pain, and improve function. Many chiropractors also use soft tissue techniques, ultrasound, electrical stimulation, and some incorporate exercise. The visit structure is often shorter and more frequent than PT, with patients sometimes seen three times weekly over extended periods.
The traditional chiropractic model frames back pain primarily as a structural alignment problem, addressed through repeated adjustment. More contemporary chiropractors take a broader view that incorporates lifestyle, exercise, and multimodal care.
What the Evidence Actually Shows
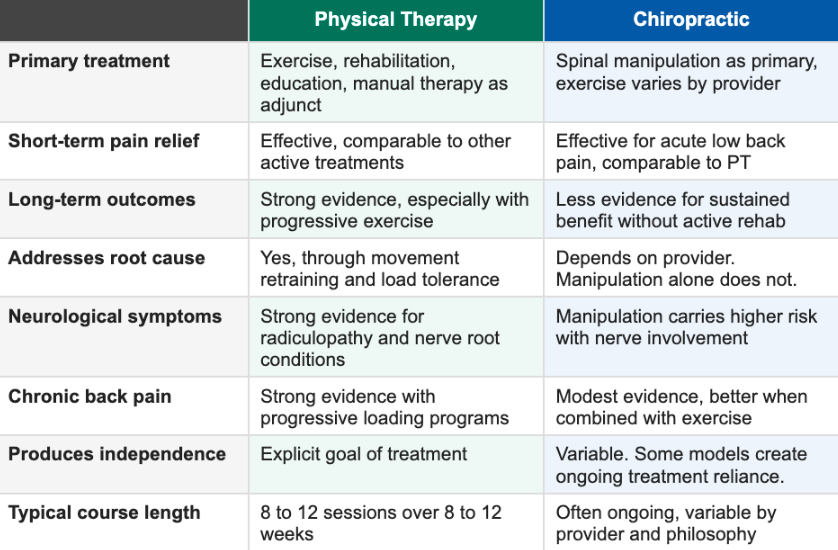
The research on spinal manipulation for acute low back pain is genuinely positive. Some research shows it produces pain relief comparable to NSAIDs and other conservative treatments in the short term. It is a real intervention with real effects.
The research on long-term outcomes is more mixed. Studies that follow patients beyond three to six months consistently find that manipulation alone, without an active rehabilitation component, does not produce better long-term outcomes than exercise. The patients who do best in chiropractic care are typically those who also receive exercise guidance and lifestyle education, not just adjustments.
The key finding on manipulation vs. exercise
A 2018 JAMA systematic review of spinal manipulation for low back pain found that manipulation produced small to moderate short-term improvements in pain and function comparable to other recommended therapies.
Critically, the review found no evidence that manipulation was superior to active exercise for long-term outcomes. The evidence for exercise as a long-term treatment for chronic low back pain is substantially stronger than the evidence for manipulation alone.
This does not mean manipulation is ineffective. It means exercise is the evidence-based foundation for durable improvement, regardless of which profession delivers it.
Where Each Approach Tends to Work Best
Situations where chiropractic care is a reasonable choice
Acute low back pain without neurological symptoms where short-term pain relief is the primary goal
Patients who respond well to manual therapy and want hands-on treatment as part of their care
Providers who incorporate active exercise and rehabilitation alongside manipulation
Patients who have had positive prior experiences with chiropractic and are managing a straightforward recurrence
Situations where physical therapy is the stronger choice
Chronic low back pain where long-term improvement, not just short-term relief, is the goal
Disc herniation with radiculopathy, where nerve root management requires directional preference assessment and neural mobilization
Lumbar spinal stenosis, where exercise direction is critical and manipulation of a stenotic segment carries risk
Cervicogenic headache, where upper cervical manual therapy combined with deep cervical flexor training is the evidence-based approach
Post-surgical rehabilitation requiring progressive, structured loading
Any presentation where building independent long-term capacity is the primary objective
A note on neurological symptoms
This is worth stating directly. For patients with significant radiculopathy, leg weakness, or any neurological involvement, high-velocity spinal manipulation carries meaningful risk. Manipulation of a disc herniation with active nerve root compression can worsen neural symptoms in some cases. Physical therapy's approach to nerve root conditions, including neural mobilization, directional preference exercises, and progressive loading, does not carry this risk profile.
This is not a general criticism of chiropractic. It is a specific clinical consideration that matters for a subset of back pain patients, and it is one of the reasons physical therapy is the recommended first-line approach for radiculopathy in most clinical guidelines.
The Most Important Question to Ask Either Provider
Whether you see a physical therapist or a chiropractor, one question predicts your outcome more than any other: does this provider have an explicit plan to make me less dependent on their care over time?
A PT or chiropractor who gives you a progressive exercise program, teaches you to understand your condition, and measures your progress toward functional goals is delivering evidence-based care. A provider who sees you three times a week indefinitely without a clear endpoint and without building your independent capacity is not, regardless of the profession.
The best practitioners in both fields know this. When you ask a provider what success looks like and how you will know when you are done, the answer tells you a great deal.
Key Takeaways
• Physical therapists and chiropractors have different training, different treatment philosophies, and different evidence bases. Neither is universally superior.
• Spinal manipulation has genuine short-term evidence for acute low back pain. Long-term outcomes are not meaningfully better than exercise alone.
• Exercise is the evidence-based foundation for durable improvement in back pain, regardless of which profession delivers it.
• For disc herniation with radiculopathy, stenosis, cervicogenic headache, and chronic spine conditions, physical therapy has a stronger evidence base and lower risk profile.
• The most important predictor of outcomes with either provider is whether they have an explicit plan to build your independence rather than ongoing treatment reliance.
• Both professions include excellent and poor practitioners. The individual provider and their approach matter as much as the profession.
Frequently Asked Questions
Is physical therapy or chiropractic better for back pain?
For acute low back pain without neurological symptoms, both produce comparable short-term outcomes. For chronic back pain, disc herniation with radiculopathy, stenosis, and cervicogenic headache, physical therapy has a stronger evidence base for long-term improvement. The most important variable is whether your provider incorporates active exercise and builds your independent capacity, regardless of their professional title.
Can a chiropractor fix a herniated disc?
Chiropractic care can reduce the pain associated with disc herniation. It does not fix or reverse the structural herniation itself. High-velocity manipulation of a disc herniation with active nerve root compression carries risk and is generally not recommended for that presentation. Physical therapy's approach to disc herniation, including directional preference exercises and neural mobilization, is better supported by evidence for this specific condition.
How many chiropractic or PT visits do I need for back pain?
A well-defined course of physical therapy for most spine conditions runs 8 to 12 sessions over 8 to 12 weeks, with a clear functional endpoint. Chiropractic visit frequency varies significantly by provider. Be cautious of any care model without a defined endpoint or explicit plan to transition you to independent management. Indefinite ongoing treatment without measurable progress toward discharge is not a positive sign regardless of which provider is delivering it.
Should I see a chiropractor or physical therapist first?
For straightforward acute low back pain without neurological symptoms, either is a reasonable starting point. For disc herniation with leg symptoms, cervicogenic headache, stenosis, or any presentation with neurological involvement, starting with a physical therapist is the evidence-based recommendation. If you have seen one and are not making progress after 6 to 8 weeks, the other is worth considering, or a consultation with a spine physician to reassess the diagnosis.
Do chiropractors and physical therapists ever work together?
Yes, and the best spine care often involves both. A patient might receive chiropractic manipulation for acute pain management while simultaneously doing a PT exercise program to build long-term capacity. Co-management between the two professions is increasingly common and is supported by the evidence, which shows that combined approaches outperform either in isolation for some presentations.
Ready to work with a specialist who will actually explain your options?
Book a free 15-minute discovery call with us at Spine33 Rehab. We will talk through your history, what you have tried, and whether our telehealth spine rehab program is the right fit.
spine33rehab.com | Book Your Free Call
About the Author
Dr. Connor Sheeks PT, DPT is a licensed physical therapist and the founder of Spine 33 Rehab PLLC, a cash-pay telehealth physical therapy practice specializing in virtual spine rehabilitation. He holds a Doctor of Physical Therapy (DPT) degree and has clinical experience treating chronic low back pain, lumbar disc herniation and radiculopathy, cervicogenic headache, lumbar spinal stenosis, postural dysfunction, and many other spinal pathologies. Spine33 Rehab currently serves patients in Tennessee via telehealth and is actively pursuing licenses in other states.
References
Paige NM, et al. (2017). Association of spinal manipulative therapy with clinical benefit and harm for acute low back pain: systematic review and meta-analysis. JAMA. doi:10.1001/jama.2017.3086
Hayden JA, et al. (2005). Exercise therapy for treatment of non-specific low back pain. Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD000335.pub2
Coulter ID, et al. (2018). Manipulation and mobilization for treating chronic low back pain: a systematic review and meta-analysis. Spine Journal. doi:10.1016/j.spinee.2018.01.013
Foster NE, et al. (2018). Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet. doi:10.1016/S0140-6736(18)30489-6