
How Long Does It Take to Recover from a Herniated Disc? A Realistic Timeline
Written by Connor Sheeks PT, DPT · Published June 2026 · Last reviewed June 2026
Reading time: approximately 9 minutes

If you have just been diagnosed with a herniated disc, the first question most people ask is not what treatment do I need. It is how long is this going to take.
It is a reasonable question, and it deserves a direct answer. The problem is that most of what you will find online is either vaguely reassuring or alarmingly open-ended. Six weeks to six months. It depends. Everyone is different.
Those answers are not wrong, but they are not useful. What actually helps is understanding the phases of disc herniation recovery, what drives the timeline in each phase, which factors are in your control, and what realistic expectations look like for your specific situation.
This article gives you that. No false optimism, no unnecessary alarm. Just an honest, evidence-based breakdown of what disc herniation recovery actually looks like and what you can do to give yourself the best possible timeline.
What you will learn in this article
• The biology of disc herniation recovery and why it takes the time it does
• A phase-by-phase recovery timeline with realistic expectations for each stage
• The factors that meaningfully speed or slow recovery
• What a good rehabilitation program looks like at each phase
• How to tell whether you are progressing normally or hitting a plateau
• When symptoms warrant surgical evaluation
• What long-term maintenance looks like after recovery
Why Recovery Takes the Time It Does: The Biology
Understanding the timeline starts with understanding what is actually happening in your body during recovery. Disc herniation recovery is not just about pain subsiding. It involves two parallel biological processes that unfold over different timeframes.
The inflammatory process
When disc material herniates and contacts a nerve root, it triggers an acute inflammatory response. The herniated nucleus pulposus contains inflammatory mediators that directly sensitize the nerve root and surrounding tissues. This chemical irritation is a primary driver of acute radicular pain and is often more significant than the mechanical compression itself.
The inflammatory phase is most intense in the first two to four weeks. As the immune system contains and begins to clear the inflammatory response, nerve root sensitivity typically begins to decrease and symptoms start to centralize, meaning leg pain retreats toward the back, which is one of the most reliable positive prognostic signs in disc herniation recovery.
Spontaneous disc reabsorption
As we covered in detail in our disc herniation article, the immune system recognizes extruded disc material as foreign tissue and actively works to reabsorb it. This process is well documented in the research and explains why disc herniations frequently shrink significantly or disappear entirely on follow-up imaging without surgery.
The reabsorption timeline varies by herniation type. Disc extrusions, where nucleus material breaks through the outer annular ring, show the highest reabsorption rates, with studies reporting complete resolution in up to 43% of cases. This process unfolds over weeks to months. Most structural reabsorption occurs within the first three to six months, though some cases continue reabsorbing for up to 12 to 18 months.
Why the worst herniations often recover fastest
Larger disc extrusions and sequestrations, the types that sound most alarming on an MRI report, have the highest rates of spontaneous reabsorption. The immune system mounts a more aggressive response to more extruded material. A 2017 systematic review found that sequestrated disc fragments showed reabsorption rates of over 96%, and extrusions showed over 90% reabsorption. Contained protrusions, the smaller and seemingly less severe type, actually showed lower reabsorption rates.
This is one of the reasons surgical urgency is not always proportional to how bad the MRI looks.
The Recovery Timeline: Phase by Phase
Most patients with acute symptomatic lumbar disc herniation move through four recognizable phases. The timelines below reflect the evidence for patients receiving appropriate conservative care, meaning active physical therapy rather than rest alone.
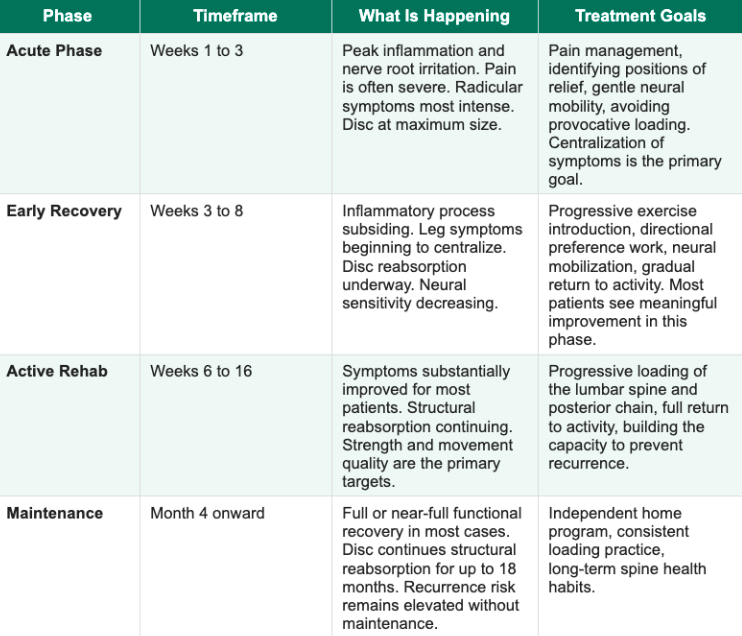
A few important clarifications about this timeline. First, it is not linear. Most patients experience days that feel like regression even when the overall trend is improvement. This is normal and should not be interpreted as the treatment failing or the condition worsening. Second, these timelines represent the evidence for acute disc herniation with radiculopathy. Chronic disc herniation presentations, where symptoms have been present for many months before treatment begins, typically take longer than these ranges suggest.
What Centralization Means and Why It Matters
Centralization is one of the most important concepts in disc herniation recovery and one that most patients are never explained. It refers to the phenomenon where leg pain, in response to specific movements or positions, retreats toward the spine. Pain that was previously felt in the foot moves to the calf. Pain in the calf moves to the thigh. Pain in the thigh moves to the lower back.
Centralization is a positive prognostic indicator with a strong evidence base. Research by McKenzie and Donelson demonstrated that patients whose symptoms centralize with treatment have significantly better outcomes than those whose symptoms do not centralize or whose pain peripheralizes (moves further down the leg). Identifying the movement direction that produces centralization, typically lumbar extension for posterior disc herniations, is one of the primary tasks of early physical therapy.
What to watch for in your own recovery
Positive signs you are progressing well:
• Leg pain retreating toward the back (centralization)
• Decreased frequency or intensity of severe pain episodes
• Improved tolerance for walking and light activity
• Symptoms that are easier to manage with position changes
Signs worth discussing with your therapist:
• Leg pain spreading further down the limb (peripheralization)
• New weakness in the leg or foot
• Symptoms unchanged after 6 to 8 weeks of consistent rehab
• Any bladder or bowel changes alongside back and leg symptoms (seek care urgently)
Factors That Meaningfully Affect Your Timeline
Recovery timelines are not random. Several well-documented factors consistently speed or slow disc herniation recovery, and a meaningful number of them are within your control.
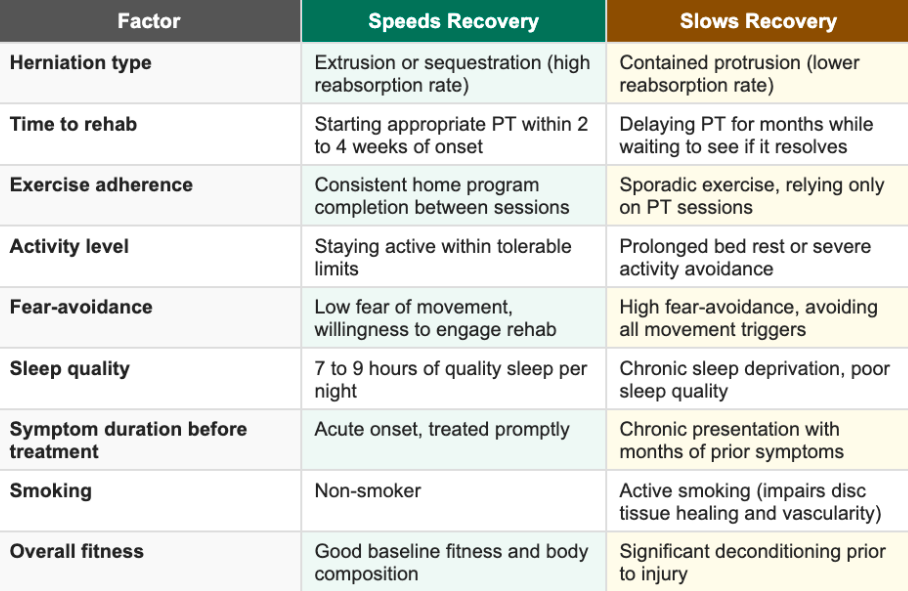
Two of these factors deserve particular attention because they are both highly impactful and highly modifiable.
Fear-avoidance is one of the strongest predictors of prolonged recovery
The fear-avoidance model is well established in the disc herniation literature. Patients who develop significant fear of movement, who interpret pain as a signal of tissue damage rather than nerve sensitivity, and who organize their lives around protecting their spine consistently show longer recovery timelines and higher rates of chronic disability than patients with equivalent structural findings who engage with active rehabilitation.
Understanding that nerve root pain is not the same as tissue damage, that movement is safe and necessary, and that symptoms are expected to fluctuate during recovery without signaling a setback are not just reassuring messages. They are evidence-based clinical interventions that change outcomes.
Sleep quality directly affects recovery speed
Sleep deprivation increases inflammatory cytokine levels, reduces pain thresholds, and impairs tissue repair processes. Research on musculoskeletal recovery consistently identifies poor sleep as a significant predictor of prolonged recovery and chronic pain development. If you are sleeping poorly because of disc pain, optimizing sleep position, using appropriate pillow support, and discussing short-term sleep management with your provider is a clinically meaningful part of your recovery plan.
What Good Rehabilitation Looks Like at Each Phase
Acute Phase: Weeks 1 to 3
The goal in this phase is not aggressive treatment. It is managing the inflammatory response, identifying positions of relief, and introducing the gentlest forms of neural mobility work that the patient can tolerate. Directional preference assessment, finding the movement direction that centralizes symptoms, is the most important clinical task.
For most posterior disc herniations, lumbar extension positions provide relief. For some, flexion is more comfortable. Attempting to force a direction that peripheralizes symptoms during this phase is counterproductive. Rest breaks in positions of relief, gentle walking within tolerance, and avoiding sustained provocative postures are the primary acute management tools.
Early Recovery Phase: Weeks 3 to 8
As symptoms begin to centralize and nerve sensitivity decreases, the rehabilitation program advances toward more active exercise. Neural mobilization techniques, which gently restore mobility and reduce mechanosensitivity of the affected nerve root, become a central component. Directional preference exercises progress in load and repetition. Walking tolerance typically improves meaningfully during this phase for most patients.
This is also the phase where patients most commonly make the mistake of stopping rehab because they feel significantly better. Feeling better and being fully recovered are not the same thing. The structural reabsorption and tissue adaptation that prevents recurrence is still underway. Stopping exercise at eight weeks because the leg pain is gone is one of the most common contributors to recurrence within 12 months.
Active Rehabilitation Phase: Weeks 6 to 16
With radicular symptoms substantially improved, the focus shifts to progressive loading of the lumbar spine and posterior chain. This is where the work that prevents recurrence happens. Strengthening the muscles that support the lumbar spine under load, restoring full movement quality, and systematically returning to all activities including exercise, lifting, and sport-specific demands.
The common clinical error in this phase is keeping the program too conservative for too long out of caution. The spine is designed to be loaded. Progressive loading is how the disc, muscles, and supporting structures rebuild tolerance. A program that stays in the gentle exercise range indefinitely does not produce the adaptation that protects against future episodes.
Maintenance: Month 4 and Beyond
Most patients are functionally recovered by month three to four but structurally still completing the reabsorption process. The maintenance phase involves transitioning from a formal PT program to an independent exercise practice that the patient owns and sustains. This is not optional. The research on recurrence rates for disc herniation is sobering: without a sustained loading practice, recurrence within one to two years is common.
The maintenance program does not need to be intensive. A consistent three to four times weekly exercise routine that includes progressive lumbar loading is sufficient for most patients. The key is consistency over intensity.
How to Tell If You Are Progressing or Plateauing
Recovery from disc herniation is not linear day to day, but it should show a clear trend over weeks. Here is how to assess whether you are on track.
You are progressing normally if:
Leg symptoms are gradually retreating toward the back over weeks
The severity of your worst pain episodes is decreasing over time
Your tolerance for walking and daily activity is increasing
You have more good days than bad days and the ratio is improving
Specific exercises reliably centralize your symptoms
You may be plateauing if:
Symptoms have not changed meaningfully in four to six weeks of consistent rehab
Leg symptoms are unchanged or spreading further down the limb
You cannot identify any movement or position that reliably provides relief
Leg weakness is present and not improving
A plateau does not automatically mean surgery. It means the current approach needs reassessment. A different directional approach, a modification to the exercise program, or evaluation for whether additional factors are contributing (sleep, stress, fear-avoidance) is the appropriate next step before escalating to procedural intervention.
When to Consider Surgical Evaluation
The vast majority of patients with lumbar disc herniation do not need surgery. For those who do, the appropriate indications are specific:
Cauda equina syndrome: loss of bladder or bowel control, saddle area numbness, or rapidly progressive bilateral leg weakness. This is a surgical emergency requiring immediate evaluation.
Progressive neurological deficit: leg weakness that is measurably worsening over days to weeks despite conservative care
Severe, unremitting radiculopathy unresponsive to 6 to 12 weeks of quality conservative treatment
Surgery is not indicated for pain alone without neurological involvement, for MRI findings without corresponding clinical symptoms, or as a first-line treatment before a genuine trial of physical therapy. Patients who pursue surgery without completing quality conservative care do not achieve better long-term outcomes in the majority of randomized controlled trials, and surgery carries real risks that must be weighed against those outcomes.
Seek immediate medical evaluation if you experience:
• Loss of bladder or bowel control
• Numbness in the groin, inner thighs, or saddle area
• Rapidly progressive leg weakness in one or both legs
• Back pain with fever or unexplained weight loss
These symptoms may indicate cauda equina syndrome, a medical emergency.
Key Takeaways
• Disc herniation recovery involves two parallel processes: resolution of nerve root inflammation and spontaneous reabsorption of disc material. Both take time.
• Most patients with acute symptomatic disc herniation experience meaningful improvement within 6 to 12 weeks of appropriate conservative care
• Centralization of symptoms, leg pain retreating toward the spine, is the most reliable positive prognostic sign in recovery
• The largest herniations often have the highest reabsorption rates, MRI severity does not determine prognosis as directly as most patients assume
• Fear-avoidance and sleep quality are two of the most modifiable factors that affect recovery speed
• Stopping rehabilitation when symptoms improve is one of the most common causes of recurrence. Full structural recovery continues well beyond pain resolution
• Surgery is appropriate for cauda equina syndrome, progressive neurological deficit, or severe radiculopathy unresponsive to 6 to 12 weeks of quality conservative care
• A sustained independent exercise practice after formal PT ends is the primary protector against recurrence
Frequently Asked Questions
How long does a herniated disc take to heal without surgery?
Most patients with acute symptomatic disc herniation experience significant improvement within 6 to 12 weeks of appropriate conservative care. Structural reabsorption of the herniated material can continue for up to 12 to 18 months. Full functional recovery, meaning return to all activities without significant limitation, typically occurs within three to six months for most patients. Chronic presentations with longer symptom duration before treatment take correspondingly longer.
Can a herniated disc heal completely?
For many patients, yes. Research demonstrates that disc herniations, including significant extrusions, frequently undergo complete or near-complete spontaneous reabsorption. A 2017 systematic review found reabsorption rates of over 90% for extrusions and over 96% for sequestrations. Complete resolution of symptoms alongside structural reabsorption is achievable for a meaningful proportion of patients, particularly those who engage with appropriate rehabilitation early.
What speeds up herniated disc recovery?
Starting appropriate physical therapy early rather than waiting, staying active within tolerable limits rather than resting, addressing fear-avoidance around movement, optimizing sleep quality, maintaining consistent exercise between therapy sessions, and not stopping rehabilitation prematurely when symptoms improve. These factors are all well-supported in the literature as predictors of faster and more complete recovery.
Is it normal for disc herniation pain to come and go during recovery?
Yes, and this is one of the most important things to understand about the recovery process. Day-to-day fluctuation in symptoms is completely normal and does not indicate that treatment is failing or that the condition is worsening. What matters is the trend over weeks, not the variation day to day. More good days than bad days, with the overall severity and frequency of severe episodes decreasing over time, is the trajectory to track.
When can I return to exercise with a herniated disc?
Light activity, including walking and gentle exercise, should begin as soon as tolerable, even in the acute phase. The goal is not rest. It is graded, progressive return to activity guided by symptoms. Most patients can return to structured gym exercise during the early recovery phase, typically weeks three to eight, with appropriate program modification. Return to heavier loading, including deadlifts, squats, and carries, is typically appropriate in the active rehabilitation phase with proper technique and progressive loading.
My symptoms improved and then got worse again. Is that normal?
A temporary worsening following a period of improvement, sometimes called a flare, is common in disc herniation recovery and does not necessarily mean you are back at square one. Flares can be triggered by activity, position, stress, or poor sleep, and they typically resolve more quickly than the original episode. If a flare persists beyond a week or two without returning toward your baseline, or if you notice new neurological symptoms like increasing leg weakness, that warrants reassessment with your therapist.
Dealing with a herniated disc and not sure where you are in your recovery?
Book a free 15-minute discovery call with us at Spine33 Rehab. We will talk through your timeline, your symptoms, and whether a telehealth spine rehab program is the right next step for you.
spine33rehab.com | Book Your Free Call
About the Author
Dr. Connor Sheeks PT, DPT is a licensed physical therapist and the founder of Spine 33 Rehab PLLC, a cash-pay telehealth physical therapy practice specializing in virtual spine rehabilitation. He holds a Doctor of Physical Therapy (DPT) degree and has clinical experience treating chronic low back pain, lumbar disc herniation and radiculopathy, cervicogenic headache, lumbar spinal stenosis, postural dysfunction, and many other spinal pathologies. Spine33 Rehab currently serves patients in Tennessee via telehealth and is actively pursuing licenses in other states.
References
Chiu CC, et al. (2015). The probability of spontaneous regression of lumbar herniated disc: a systematic review. Clinical Rehabilitation. doi:10.1177/0269215514540919
Suri P, et al. (2012). Does this patient have lumbar spinal stenosis? JAMA. doi:10.1001/jama.2010.553
Werneke MW, Hart DL. (2001). Centralization phenomenon as a prognostic factor for chronic low back pain and disability. Spine. doi:10.1097/00007632-200111150-00012
Leeuw M, et al. (2007). The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. Journal of Behavioral Medicine. doi:10.1007/s10865-006-9085-0
Deyo RA, Mirza SK. (2016). Herniated lumbar intervertebral disk. New England Journal of Medicine. doi:10.1056/NEJMcp1512658
Jensen TS, et al. (2006). Prediction of future low back pain based on MRI findings in a cohort of 40-year-old Danes. Spine. doi:10.1097/01.brs.0000228839.op