
Neck Pain from Screen Time: What Is Actually Happening in Your Spine
Written by Connor Sheeks PT, DPT · Published June 2026 · Last reviewed June 2026
Reading time: approximately 8 minutes

You sit down to work, feel fine. Two hours later your neck aches. By the end of the day it is stiff, your shoulders are tight, and there is a dull pressure at the base of your skull that may or may not become a headache. You stretch, feel better for a while, and repeat the whole cycle the next day.
This pattern is not random and it is not inevitable. It has a specific anatomical explanation, predictable contributing factors, and a clear evidence-based path to resolving it. Most people who experience it spend months managing symptoms day to day without ever addressing what is actually causing them.
This article explains the mechanics of screen-related neck pain, which structures are involved, why the problem tends to persist without the right intervention, and what actually changes outcomes.
What you will learn in this article
The anatomy of why screen time loads your neck the way it does
Which specific structures are most commonly involved
Why stretching provides temporary relief but not lasting change
The connection between neck pain and headaches in screen workers
What workstation factors actually matter and which ones do not
What an effective rehabilitation program targets
When neck pain from screen time warrants clinical evaluation
The Mechanics: What Screen Time Actually Does to Your Cervical Spine
The average adult head weighs between 10 and 12 pounds in neutral alignment, balanced directly over the shoulders. As the head translates forward from neutral, the effective load on the cervical spine increases substantially. Research by Hansraj (2014) estimated that at 15 degrees of forward head flexion the effective load increases to approximately 27 pounds. At 30 degrees, approximately 40 pounds. At 60 degrees, the position many people adopt when looking at a phone or a low monitor, the effective load approaches 60 pounds.
This is not a catastrophic structural event. The cervical spine is designed to tolerate load. The problem is duration and repetition. Sustaining that elevated load across a full workday, five days a week, in tissues that are not conditioned to handle it, produces the cumulative fatigue, sensitization, and muscle imbalance pattern that becomes chronic neck pain.
What happens to cervical tissues under sustained load
Muscle fatigue: the deep cervical flexors (longus colli, longus capitis) fatigue under sustained forward head loading, shifting demand to the superficial cervical muscles and upper trapezius, which are not designed for sustained postural work
Creep: viscoelastic tissues including the posterior cervical ligaments and joint capsules undergo gradual deformation under sustained load, reducing their stiffness and load tolerance over time.
Joint compression: sustained forward head posture increases compressive load on the posterior cervical facet joints, particularly at C4 to C6, which are the most commonly symptomatic segments in screen workers.
Neural sensitization: chronic tissue loading produces local inflammatory mediators that sensitize nearby nerve endings, lowering the pain threshold and making tissues that were previously comfortable become symptomatic.
Which Structures Are Most Commonly Involved
The deep cervical flexors
The deep cervical flexors, longus colli and longus capitis, are the primary segmental stabilizers of the cervical spine. They run along the front of the cervical vertebrae and are responsible for maintaining the cervical lordosis and controlling segmental motion under load. Research consistently demonstrates that people with chronic neck pain, including screen-related neck pain, show measurably impaired deep cervical flexor endurance and delayed neuromuscular activation compared to pain-free controls.
When the deep flexors fatigue or are underactive, the superficial neck muscles including the upper trapezius, sternocleidomastoid, and scalenes compensate. These muscles are designed for movement, not sustained postural work. Their chronic overactivation produces the familiar pattern of tight, tender upper trapezius and levator scapulae that most screen workers recognize.
The cervical facet joints
The posterior facet joints of the cervical spine, particularly C4 to C6, are frequently the primary pain generators in persistent screen-related neck pain. Sustained forward head posture increases compressive and shear loading on these joints. Over time this produces local joint irritation, restricted segmental mobility, and referred pain into the surrounding musculature.
Facet joint referral patterns from the cervical spine are predictable: C2 to C3 refers to the suboccipital region and can produce headache. C3 to C4 refers to the posterior neck and shoulder girdle. C4 to C5 refers to the trapezius region. C5 to C6 refers to the shoulder and lateral arm. Understanding these patterns helps explain why screen workers often report pain well beyond the neck itself.
The suboccipital region
The suboccipital muscles at the base of the skull are chronically overloaded in forward head posture. As the head translates forward, the suboccipital muscles must work harder to maintain horizontal gaze, placing them under sustained tension that produces local tenderness, restricted upper cervical mobility, and in many cases the referred headache pattern characteristic of cervicogenic headache.
For a detailed explanation of how this produces headaches, see our article on neck pain and cervicogenic headaches.
The thoracic spine
Thoracic spine stiffness is one of the most consistent and most overlooked findings in screen workers with neck pain. The thoracic spine and cervical spine work as a mechanical unit. When thoracic extension mobility is restricted, the cervical spine must compensate by moving into greater extension to maintain posture and horizontal gaze. This compensation increases cervical joint loading and reduces the available range of movement before symptoms occur.
Addressing thoracic mobility as part of neck pain rehabilitation consistently improves cervical range of motion and reduces symptoms, even without directly treating the cervical spine. This is one of the higher-yield interventions in screen-related neck pain management.
Why Stretching Helps Temporarily but Not Long-Term
Most people with screen-related neck pain have tried stretching. It works, for a while. The neck feels looser, the tension releases, and within a few hours the same pattern returns.
The reason is straightforward: stretching addresses the symptom, which is muscle tension, without addressing the cause, which is insufficient capacity in the cervical stabilizers to handle the daily postural load being placed on them. A muscle that is tight because it is compensating for an underactive deep stabilizer will return to that compensatory state as soon as the load is reapplied.
Stretching the upper trapezius without strengthening the deep cervical flexors is the equivalent of repeatedly draining a bathtub without turning off the tap. Temporary relief, no lasting change.
The Headache Connection
A meaningful proportion of screen workers with neck pain also experience headaches that they attribute to eye strain, stress, or tension. Many of these headaches are cervicogenic in origin, meaning they are generated by the same upper cervical structures that produce the neck pain, not by a separate process.
The clinical indicators that suggest a screen-related headache is cervicogenic rather than tension or migraine include onset at the base of the skull, one-sided distribution, worsening with sustained screen posture or neck movement, and relief with positions that reduce cervical loading. If this pattern describes your headaches, treating the cervical spine is the appropriate intervention, not headache medication.
For a full breakdown of cervicogenic headache diagnosis and treatment, see our article on neck pain and cervicogenic headaches.
What Workstation Factors Actually Matter
Ergonomic advice for screen workers is abundant and often over-specified. The research on which workstation factors actually predict neck pain outcomes is more selective than the typical ergonomic checklist suggests.
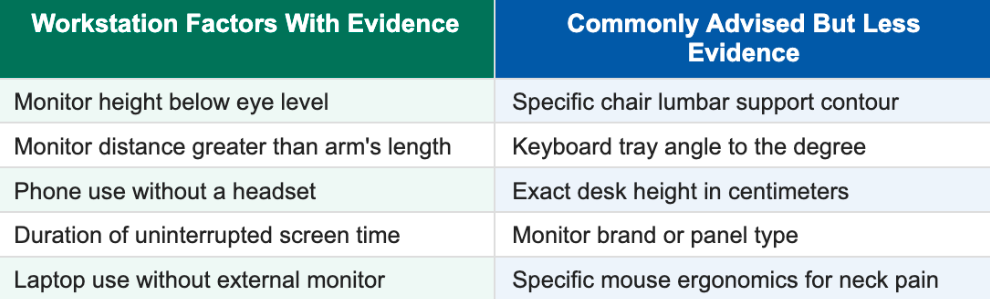
The factors with the strongest evidence are those that directly drive sustained forward head loading: a monitor positioned too low (forcing sustained cervical flexion), prolonged uninterrupted screen sessions without position changes, and phone use without a headset (which forces sustained lateral cervical flexion and rotation).
The most important workstation intervention for most screen workers is not a specific ergonomic adjustment. It is increasing position variability and reducing the duration of sustained static postures. Moving regularly matters more than achieving a perfect static setup.
Practical workstation adjustments with the strongest impact
Raise your monitor so the top of the screen is at or slightly below eye level
Position your monitor at arm's length or slightly further
Use a headset or speakerphone for calls lasting more than a few minutes
Set a movement reminder every 30 to 45 minutes
If using a laptop as your primary screen, add an external monitor or stand
Keep your phone at eye level when reading rather than looking down
What an Effective Rehabilitation Program Targets
Workstation adjustments reduce the load being placed on the cervical spine. Rehabilitation builds the capacity to handle that load. Both are necessary. Neither alone is sufficient for most people with established neck pain.
Deep cervical flexor strengthening
Craniocervical flexion training, the specific protocol targeting the longus colli and longus capitis, is the most evidence-supported exercise intervention for screen-related neck pain and cervicogenic headache. It involves graduated activation of the deep cervical flexors through precise, low-load movements performed with biofeedback or careful technique cueing.
This is not a standard chin tuck exercise. The depth of activation, the range of motion used, and the progression protocol matter significantly for outcomes. Done correctly, consistent deep flexor training over 6 to 8 weeks produces measurable improvements in pain, function, and headache frequency in screen workers.
Thoracic mobility work
Thoracic extension and rotation mobilization is a high-yield early intervention that consistently improves cervical range of motion and reduces neck pain, often before the cervical spine itself is directly treated. Foam rolling the thoracic spine, thoracic extension over a roller or rolled towel, and rotational mobility exercises are practical starting points that can be performed at home or at the workstation.
Cervical strengthening and endurance
Beyond the deep flexors, building endurance in the lower trapezius, middle trapezius, and serratus anterior addresses the scapular stability deficits that contribute to upper trapezius overload in screen workers. The upper trapezius becomes overactive partly because the lower trapezius and serratus are underactive. Addressing this imbalance reduces the chronic tension in the upper neck and shoulder region.
Movement habits
The most durable long-term change for screen workers is not a specific exercise. It is building the habit of regular position changes, brief mobility breaks, and varying how the cervical spine is loaded throughout the day. Structured movement breaks of 2 to 3 minutes every 30 to 45 minutes consistently outperform ergonomic optimization alone in research on screen worker neck pain.
When to Seek Clinical Evaluation
Screen-related neck pain that follows the pattern described in this article, aching and stiffness that builds across the day and improves with rest and movement, is appropriate for self-management with the strategies above and for physical therapy.
The following presentations warrant clinical evaluation:
Neck pain with arm pain, numbness, or tingling radiating below the elbow
Neck pain with progressive arm or hand weakness
Severe headaches that are new in pattern or accompanied by neurological symptoms
Neck pain following trauma, even minor
Neck pain with fever, unexplained weight loss, or night sweats
Symptoms that have not improved after 6 to 8 weeks of appropriate self-management
Arm symptoms below the elbow can suggest cervical radiculopathy, where a nerve root in the neck is being compressed or irritated. This is a different clinical picture from screen-related neck pain and requires a specific diagnostic evaluation and targeted treatment approach.
Key Takeaways
Sustained forward head posture during screen use progressively increases cervical spine loading, producing cumulative fatigue and sensitization in the deep cervical flexors, facet joints, and suboccipital region
The deep cervical flexors are the primary cervical stabilizers and are consistently underactive in people with screen-related neck pain. Their fatigue drives compensatory overactivity in the upper trapezius and surrounding muscles
Stretching provides temporary relief but does not address the underlying cause. Building deep cervical flexor capacity is the primary rehabilitation target
Thoracic spine stiffness is a consistent and underappreciated contributor to screen-related neck pain. Thoracic mobility work reliably improves cervical symptoms
Many screen worker headaches are cervicogenic in origin, generated by the same upper cervical structures producing the neck pain
The most impactful workstation interventions are monitor height, reducing uninterrupted screen duration, and increasing position variability throughout the day
Arm symptoms below the elbow, progressive weakness, or neurological symptoms alongside neck pain warrant prompt clinical evaluation
Frequently Asked Questions
Why does my neck hurt after working at a computer?
Sustained screen use places the cervical spine in forward head posture, increasing the effective load on the cervical muscles, joints, and ligaments progressively over the course of the day. The deep cervical flexors fatigue under this load, shifting demand to superficial compensator muscles that are not designed for sustained postural work. The result is the familiar pattern of increasing neck tension, stiffness, and aching that builds across a workday.
Is neck pain from screen time serious?
Screen-related neck pain without neurological symptoms is not structurally serious, but it can become chronic and significantly impact quality of life and work function if the underlying drivers are not addressed. The pattern tends to worsen progressively without intervention as deconditioning and movement restriction develop over months. Early rehabilitation produces better outcomes than waiting until the pain is severe.
What is the best exercise for neck pain from computer use?
Deep cervical flexor training, specifically craniocervical flexion training targeting the longus colli and longus capitis, has the strongest evidence for screen-related neck pain. Combined with thoracic extension mobility work, this approach addresses the two primary contributors to screen worker neck pain. Stretching alone is not sufficient as a primary intervention and should be used as a complement to strengthening, not a substitute.
How should I set up my monitor to reduce neck pain?
Raise your monitor so the top of the screen is at or just below eye level. Position it at arm's length or slightly further. If you use a laptop as your primary screen, add an external monitor or laptop stand and external keyboard. These adjustments reduce the degree of sustained cervical flexion during screen use. Equally important is taking movement breaks every 30 to 45 minutes regardless of your monitor height.
Can a standing desk fix neck pain?
A standing desk can increase position variability, which is beneficial. However, standing in the same forward head posture you used when sitting, which is common, produces the same cervical loading. The benefit of a standing desk for neck pain specifically depends on whether it changes your head position relative to the screen. If you raise the monitor appropriately when standing, it can help. If the screen remains at the same height, the benefit for neck pain is limited.
When should I see a physical therapist for neck pain?
If your neck pain has been present for more than 4 to 6 weeks without meaningful improvement, is accompanied by headaches that have not responded to typical headache management, or is beginning to affect your work productivity or daily function, a physical therapy evaluation is appropriate. Arm symptoms, including pain, numbness, or tingling below the elbow, warrant evaluation sooner rather than later.
Neck pain that follows you home from the screen? Let us take a look.
Book a free 15-minute discovery call with us at Spine33 Rehab. We will review your history, your work setup, and whether our telehealth spine rehab program is the right fit for what you are dealing with.
spine33rehab.com | Book Your Free Call
About the Author
Dr. Connor Sheeks PT, DPT is a licensed physical therapist and the founder of Spine 33 Rehab PLLC, a cash-pay telehealth physical therapy practice specializing in virtual spine rehabilitation. He holds a Doctor of Physical Therapy (DPT) degree and has clinical experience treating chronic low back pain, lumbar disc herniation and radiculopathy, cervicogenic headache, lumbar spinal stenosis, postural dysfunction, and many other spinal pathologies. Spine33 Rehab currently serves patients in Tennessee via telehealth and is actively pursuing licenses in other states.
References
Hansraj KK. (2014). Assessment of stresses in the cervical spine caused by posture and position of the head. Surgical Technology International. PMID: 25393825
Falla DL, Jull GA, Hodges PW. (2004). Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles during performance of the craniocervical flexion test. Spine. doi:10.1097/01.brs.0000146464.40684.7f
Gross A, et al. (2015). Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD004249.pub4
Hallman DM, et al. (2016). Computer use, neck and shoulder pain and the role of workplace physical activity. Applied Ergonomics. doi:10.1016/j.apergo.2015.07.018
Jull G, et al. (2009). Therapeutic exercise for the cervical spine. In: Jull G, Sterling M, Falla D, Treleaven J, O'Leary S (Eds), Whiplash, Headache and Neck Pain. Elsevier.