
Lumbar Spinal Stenosis: The Exercises That Help (And the Ones That Make It Worse)
Written by Connor Sheeks, PT DPT · Published May 2026 · Last reviewed May 2026
Reading time: approximately 9 minutes

If you have lumbar spinal stenosis, you have probably noticed that not all movement feels the same. Walking a few blocks leaves your legs heavy and achy. Standing in line at the grocery store is surprisingly difficult. But sitting down, leaning forward over a shopping cart, or riding a stationary bike feels noticeably better.
That pattern is not random. It is a direct reflection of the anatomy of stenosis, and understanding it is the key to knowing which exercises will help you and which ones will make your symptoms worse.
This matters more for stenosis than almost any other spine condition. Unlike disc herniation, where the wrong exercise might simply not help, the wrong exercise direction for stenosis can actively increase nerve compression and worsen symptoms. Getting this right is not optional.
This article explains what lumbar spinal stenosis is, why symptoms behave the way they do, which exercises and activities are supported by evidence, and which ones you should avoid.
What you will learn in this article
• What lumbar spinal stenosis is and why it causes the symptoms it does
• Why your symptoms get better when you sit and worse when you stand or walk
• The exercises with the strongest evidence for stenosis
• The exercises and positions that worsen stenosis symptoms
• How physical therapy addresses stenosis specifically
• What realistic management looks like over time
• When stenosis requires surgical evaluation
What Lumbar Spinal Stenosis Actually Is
Lumbar spinal stenosis is a narrowing of the spaces within the lumbar spine through which the spinal cord, nerve roots, or both must pass. That narrowing can occur in three locations:
Central stenosis: narrowing of the main spinal canal, where the cauda equina nerve roots travel.
Foraminal stenosis: narrowing of the openings through which individual nerve roots exit the spine.
Lateral recess stenosis: narrowing of the lateral portions of the spinal canal where nerve roots travel before exiting.
The narrowing is caused by the cumulative effects of spinal aging: disc degeneration and height loss, bone spur formation on the vertebral bodies and facet joints, thickening and buckling of the ligamentum flavum (the ligament running along the back of the spinal canal), and facet joint hypertrophy. All of these changes reduce the available space for neural structures.
Lumbar stenosis is primarily a condition of aging. It is uncommon before 50 and becomes progressively more prevalent with each decade. It is one of the most common reasons for spine surgery in adults over 65.
Central canal vs. foraminal stenosis: does the distinction matter?
Yes, clinically. Central stenosis primarily causes neurogenic claudication (bilateral leg symptoms with walking and standing). Foraminal stenosis tends to produce more unilateral radicular symptoms similar to disc herniation. The two can coexist. Treatment principles overlap significantly, but identifying which type predominates helps predict which positions and exercises will provide the most relief.
Why Symptoms Behave the Way They Do
The defining symptom pattern of lumbar stenosis is neurogenic claudication: leg pain, heaviness, numbness, or weakness that comes on with walking or prolonged standing and is relieved by sitting or bending forward. Understanding why this happens makes everything else in this article make sense.
The spinal canal is not a fixed tube. Its dimensions change with movement. Lumbar extension (bending backward, standing upright, walking) causes the ligamentum flavum (a ligament connecting parts of adjacent vertebrae) to buckle inward, the facet joints to approximate, both of which reduce available canal space and increase pressure on the neural structures inside. These changes reduce the available canal space and increase pressure on the neural structures inside.
Lumbar flexion (bending forward, sitting, leaning over a shopping cart) does the opposite. It opens the posterior elements of the spine, stretches the ligamentum flavum taut, and increases canal diameter. Neural structures have more room, symptoms reduce.
Why the shopping cart sign matters
A classic clinical observation: patients with lumbar stenosis can often walk much farther when leaning forward on a shopping cart than when walking upright. This is not a strength or balance issue. It is a direct mechanical effect of lumbar flexion increasing spinal canal diameter.
The shopping cart sign is one of the most reliable clinical indicators of neurogenic claudication from lumbar stenosis. If this describes you, the flexion bias of your exercise program is not optional. It is the mechanism of relief.
The Exercises That Help: What the Evidence Supports
Effective exercise for lumbar stenosis works with the flexion bias of the condition. The goal is not just symptom management in the short term. It is improving tolerance for activity, building the muscular support that reduces mechanical load on the narrowed segments, and restoring as much functional capacity as possible.
Lumbar flexion exercises
Exercises that encourage lumbar flexion are the foundation of stenosis rehabilitation. They directly address the mechanical problem by opening the spinal canal and reducing neural compression during movement.
Posterior pelvic tilt: lying on your back, gently flattening the lower back against the floor by contracting the abdominals and glutes. Simple, low-load, and effective as an entry-level exercise and a position of relief during symptom flares.
Knees to chest: lying on your back, drawing both knees toward the chest and holding. Opens the posterior lumbar spine and provides immediate relief for many stenosis patients.
Seated lumbar flexion: sitting in a chair and slowly rounding forward, letting the chest drop toward the thighs. A useful exercise and a practical relief position during daily activities.
Child's pose (modified): a kneeling forward fold position that places the lumbar spine in sustained flexion. Excellent for symptom management and as a rest position during activity.
Stationary cycling
Stationary cycling is one of the most consistently recommended activities for lumbar stenosis, and for good reason. The seated, slightly forward-flexed position of cycling places the lumbar spine in relative flexion throughout the activity. It provides cardiovascular training, lower extremity conditioning, and hip muscle strengthening without the extension-loaded upright walking posture that provokes symptoms.
Most stenosis patients can tolerate significantly more time on a stationary bike than they can walking upright. This makes it a practical and evidence-supported cornerstone of the exercise program, particularly in the early stages when walking tolerance is limited.
Aquatic therapy
Water-based exercise is particularly effective for stenosis because buoyancy reduces the compressive load on the spine while allowing active lower extremity exercise. Many patients with limited walking tolerance on land can exercise comfortably and productively in a pool. Aquatic therapy is a strong option when land-based exercise is significantly limited by symptoms.
Hip flexor stretching
Tight hip flexors (particularly the iliopsoas) pull the lumbar spine into extension, increasing lumbar lordosis and further narrowing the spinal canal. Systematic hip flexor stretching as part of a stenosis program reduces this extension bias and is consistently included in evidence-based protocols.
Core and gluteal strengthening in neutral or flexed positions
The goal of core strengthening in stenosis is to build the muscular support that reduces the compressive and shear forces on the narrowed segments during daily activity. The important distinction from general back pain programs: stenosis patients should perform core strengthening in positions of lumbar neutral or slight flexion, not extension. Exercises like bird-dog performed with excessive lumbar extension can worsen symptoms.
Glute strengthening is also a priority. Strong hip extensors and abductors reduce the mechanical demands on the lumbar spine during walking and standing. Exercises like clamshells, side-lying hip abduction, and glute bridges (with a flat or posteriorly tilted pelvis) are well tolerated by most stenosis patients.
Walking with modification
Walking remains important for overall health and function, but stenosis patients need to modify how they walk. Shorter distances, more frequent rest breaks in a forward-flexed position (sitting, leaning on a counter), and using a walking aid that encourages slight forward lean can significantly extend walking tolerance. The goal is to keep walking as part of daily life while managing symptoms intelligently rather than pushing through worsening leg pain.
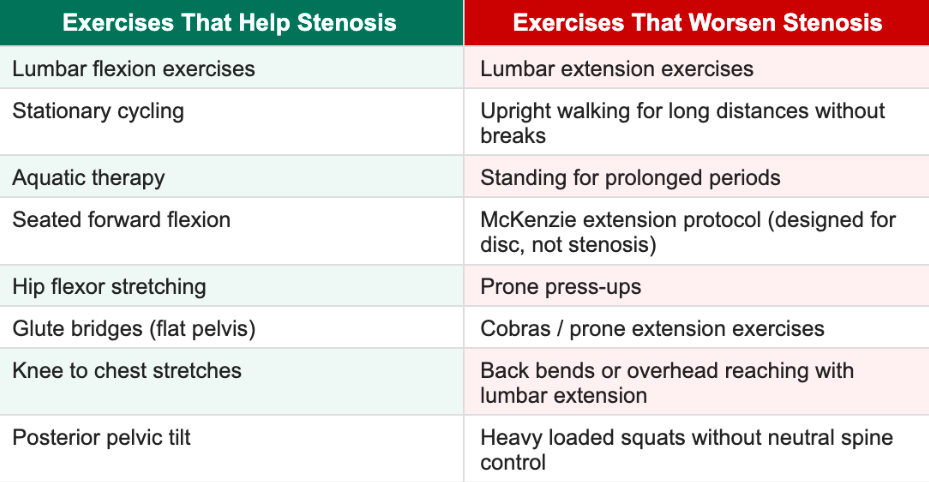
The Exercises and Positions That Make Stenosis Worse
This section is as important as the previous one. For stenosis patients specifically, here is a general guide regarding movements that can relieve and exacerbate symptoms:
The most common mistake: using extension exercises designed for disc herniation
McKenzie extension exercises (prone press-ups, repeated lumbar extension) are highly effective for disc herniation with a posterior herniation pattern. They are contraindicated for lumbar stenosis. Extension closes the spinal canal. For a disc herniation patient, this can centralize symptoms and reduce nerve pressure. For a stenosis patient, the same movement reduces canal diameter further and can worsen neural compression.
This is the most common exercise error we see in patients who have done physical therapy before for back pain and are applying the wrong protocol to a different diagnosis. If a prior PT program used extension-based exercises and your symptoms did not improve or worsened, this may be why.
What Physical Therapy Addresses Beyond Exercises
Exercise selection is important, but a comprehensive physical therapy program for lumbar stenosis addresses several additional components that exercise alone does not cover.
Activity modification and pacing. Identifying the specific activities that provoke symptoms, modifying how they are performed, and building a pacing strategy that allows you to stay active without repeatedly triggering severe symptom flares.
Postural education. Understanding which positions load the spine into extension and how to modify standing, walking, and sleeping positions to reduce symptoms throughout the day. Small changes to daily posture can meaningfully reduce cumulative neural irritation.
Manual therapy to adjacent regions. While direct mobilization of severely stenotic segments carries more risk than benefit, mobilization of the hip joints, sacroiliac region, and thoracic spine can reduce the compensatory mechanical demands placed on the lumbar segments and improve overall movement quality. Of course, this aspect of therapy would need to be in-person. If we believe you would benefit from this component of physical therapy, we will tell you.
Neurogenic claudication management. Practical strategies for extending walking tolerance: interval walking with flexion rest breaks, using a walking aid, and understanding the physiology of claudication so that symptom onset does not trigger fear or excessive activity reduction.
Long-term self-management. Stenosis does not resolve the way disc herniation often does. The goal of PT is to give you the understanding and tools to manage your own condition independently over time, with less reliance on ongoing treatment.
A note from Dr. Connor Sheeks, PT DPT
"Stenosis is one of the conditions where setting realistic expectations upfront matters most. This is not a condition we are going to cure with physical therapy. What we are going to do is significantly improve your function, extend how far you can walk, reduce how much your symptoms intrude on your daily life, and give you a framework for managing this independently. For most patients, that is a substantial quality of life improvement. For some, it delays or avoids surgery entirely. That is a meaningful outcome, and it is what the evidence supports."
What Realistic Management Looks Like
Lumbar stenosis requires a different mindset than acute conditions. It is a structural narrowing that does not reverse with conservative care. The goal of rehabilitation is optimizing function within the constraints of the anatomy.
Weeks 1 to 3: Comprehensive assessment of symptom pattern and walking tolerance. Introduction of flexion-biased exercises, stationary cycling if tolerated, activity modification strategies. Identification of positions of relief for symptom management during daily activity.
Weeks 4 to 8: Progressive increase in exercise load and volume. Hip flexor and hip strengthening progression. Walking tolerance training with structured pacing. Most patients see meaningful improvement in functional walking distance and daily symptom burden during this phase.
Weeks 8 to 12: Consolidation of gains. Transition to independent home program. Education on long-term self-management, flare-up response, and activity planning.
Beyond 12 weeks: Maintenance of a consistent exercise practice is the most important long-term variable. Stenosis patients who maintain regular activity and flexion-biased exercise consistently outperform those who rely on passive treatment or stop exercising after formal PT ends.
Most patients with moderate lumbar stenosis achieve meaningful improvement in walking tolerance, daily function, and symptom severity within 8 to 12 weeks of a well-designed program. Some achieve outcomes that make surgery unnecessary. Others use conservative care to optimize their condition before a planned surgical procedure.
When Stenosis Requires Surgical Evaluation
Surgery for lumbar stenosis has reasonable evidence for specific presentations. The primary surgical procedure is a decompression laminectomy, which removes the structures causing narrowing and creates more space for the neural elements.
Surgical evaluation is appropriate when:
Neurological deficits are progressive, including worsening leg weakness that is not stabilizing with conservative care
Walking tolerance is so severely limited that quality of life is significantly impaired and conservative care has not produced meaningful improvement after 3 to 6 months
Cauda equina symptoms are present, including bladder or bowel dysfunction or saddle area numbness, which require urgent evaluation
The patient has a specific structural instability such as spondylolisthesis that is contributing to the stenosis and may require stabilization
Surgery is not indicated for imaging findings alone, for mild to moderate symptoms that respond to conservative management, or as a first-line treatment before a genuine trial of physical therapy. Research consistently shows that patients who pursue surgery without first completing quality conservative care do not achieve better long-term outcomes than those who do.
Seek immediate medical evaluation if you experience:
Loss of bladder or bowel control
Numbness in the groin, inner thighs, or saddle area
Rapidly progressive leg weakness in both legs
Back pain with fever or unexplained weight loss
These symptoms may indicate cauda equina syndrome or another serious condition requiring emergency evaluation.
Key Takeaways
• Lumbar spinal stenosis is a narrowing of the spinal canal caused by age-related degenerative changes including disc degeneration, bone spurs, and ligament thickening
• Symptoms usually worsen with extension (standing, walking upright) and improve with flexion (sitting, leaning forward) because lumbar flexion opens the spinal canal
• Effective exercises work with the flexion bias: lumbar flexion exercises, stationary cycling, aquatic therapy, hip flexor stretching, and glute strengthening in neutral or flexed positions
• Extension exercises designed for disc herniation (prone press-ups, cobras, McKenzie extension) are contraindicated for stenosis and can worsen neural compression
• A full PT program also addresses activity modification, pacing, postural education, and long-term self-management
• Stenosis does not reverse with conservative care, but most patients achieve meaningful improvement in walking tolerance and daily function within 8 to 12 weeks of a well-designed program
• Surgery is appropriate for progressive neurological deficits, cauda equina symptoms, or severe functional limitation unresponsive to quality conservative care
Frequently Asked Questions
What is the best exercise for lumbar spinal stenosis?
There is no single best exercise, but the most consistently effective category is lumbar flexion exercise. Stationary cycling is one of the most practical and well-tolerated options for most stenosis patients because the seated, forward-flexed position keeps the spine in a symptom-reducing posture throughout the activity. A tailored program combining flexion exercises, hip strengthening, and activity modification consistently outperforms any single exercise.
Can exercise make spinal stenosis worse?
Yes, if the wrong exercises are chosen. Lumbar extension exercises, prone press-ups, and back bends reduce the diameter of the spinal canal and can worsen neural compression and symptoms in stenosis patients. These exercises are appropriate for some disc herniation presentations but are contraindicated for stenosis. This is one of the strongest arguments for working with a physical therapist who can identify the right exercise direction for your specific diagnosis.
Why can I walk farther when I lean on a shopping cart?
Because leaning forward on a cart places your lumbar spine in relative flexion, which opens the spinal canal and increases the space available for your nerve roots. This is called the shopping cart sign and it is one of the most reliable clinical indicators of neurogenic claudication from lumbar stenosis. Your exercise program should replicate this mechanical principle systematically.
Is walking good for spinal stenosis?
Yes, but with modification. Walking upright for long distances without rest breaks is one of the primary symptom triggers for stenosis. Walking in shorter intervals, taking frequent forward-flexed rest breaks, using a walking aid that encourages slight forward lean, and gradually increasing distance over time is a sustainable approach. The goal is to keep walking as part of daily life while managing symptoms intelligently, not to push through worsening leg pain.
Can physical therapy avoid surgery for spinal stenosis?
For many patients, yes. Research shows that a substantial proportion of patients with moderate lumbar stenosis who complete a quality conservative care program achieve functional outcomes comparable to surgical patients at one to two year follow-up. PT does not reverse the structural narrowing, but it improves the muscular support, activity tolerance, and movement patterns that determine how much that narrowing impacts daily function. Whether PT can replace surgery depends on the severity of your specific presentation.
How long does it take to see improvement from PT for stenosis?
Most patients notice meaningful improvement in walking tolerance and daily symptoms within 4 to 8 weeks of a consistent, appropriately designed program. A full course of care typically runs 10 to 12 weeks. Long-term maintenance of activity and home exercise is the primary predictor of sustained benefit beyond formal PT.
Living with lumbar stenosis and not sure where to start?
Book a free 15-minute discovery call with us today. We will talk through your symptoms, what has and has not worked, and whether a telehealth spine rehab program is the right next step for you.
spine33rehab.com | Book Your Free Call
About the Author
Dr. Connor Sheeks, PT, DPT is a licensed physical therapist and the founder of Spine 33 Rehab PLLC, a cash-pay telehealth physical therapy practice specializing in virtual spine rehabilitation. He holds a Doctor of Physical Therapy (DPT) degree and has clinical experience treating chronic low back pain, lumbar disc herniation and radiculopathy, cervicogenic headache, lumbar spinal stenosis, postural dysfunction, and many other spinal pathologies. Spine33 Rehab currently serves patients in Tennessee via telehealth and is actively pursuing licenses in other states.
References
Ammendolia C, et al. (2022). Nonoperative treatment for lumbar spinal stenosis with neurogenic claudication: an updated systematic review. BMJ Open. doi:10.1136/bmjopen-2021-057724
Delitto A, et al. (2015). Surgery versus nonsurgical treatment of lumbar spinal stenosis: a randomized trial. Annals of Internal Medicine. doi:10.7326/M14-1420
Minetama M, et al. (2021). Supervised physical therapy versus home exercise for patients with lumbar spinal stenosis. Spine Journal. doi:10.1016/j.spinee.2020.09.008
Backstrom KM, et al. (2011). Incidence and predictors of short and long-term outcomes after lumbar spinal stenosis surgery. Spine. doi:10.1097/BRS.0b013e31821baae3
Katz JN, Zimmerman ZE, Mass H, Makhni MC. (2022). Diagnosis and management of lumbar spinal stenosis: a review. JAMA. doi:10.1001/jama.2022.3872